P5025 - Retroperitoneal Fibrosis Presenting With Black Esophagus and Gastric Outlet Obstruction: A Multisystem Complication of a Rare Fibrosing Disorder
Ishan Antony, MD1, Vian Rifat, MBBCh2, Narinderjeet Kaur, MD, MS3, Yasmine Agha, MD4 1Beth Israel Lahey Health, Burlington, MA; 2Royal College of Surgeons in Ireland, Dublin, Dublin, Ireland; 3SUNY Downstate Health Sciences University, Brooklyn, NY; 4Lahey Hospital and Medical Center, Burlington, MA Introduction: Retroperitoneal fibrosis (RPF) is a rare fibroinflammatory disorder that typically surrounds the aorta and ureters, leading to obstructive uropathy. Gastrointestinal (GI) involvement is uncommon, with isolated reports of duodenal obstruction. We present a unique case of RPF manifesting as both gastric outlet obstruction (GOO) and acute esophageal necrosis (AEN), a convergence of severe GI complications with systemic implications.
Case Description/
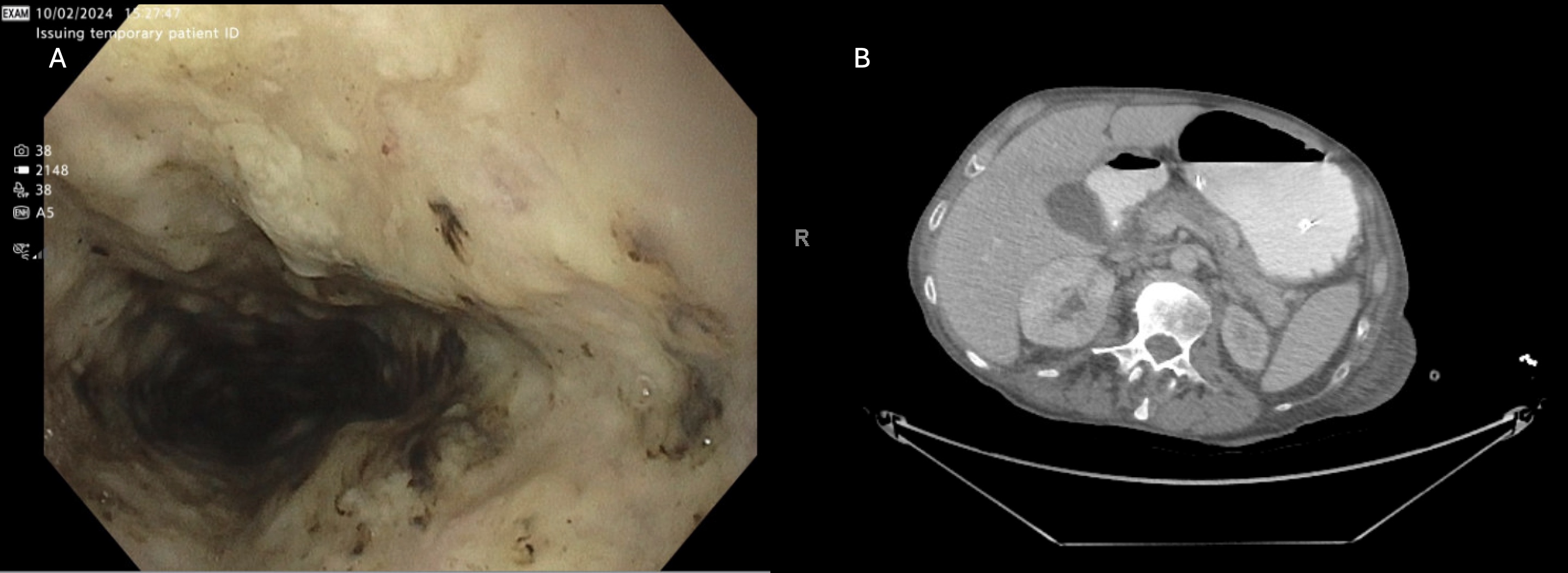
Methods: A 66-year-old woman with a history of breast cancer and known RPF (status post nephrostomy for bilateral ureteral obstruction) presented to the emergency department with fatigue and abdominal discomfort. Shortly after arrival, she experienced a witnessed cardiac arrest due to torsades de pointes, attributed to QT-prolonging medications (fluoroquinolone, Paxlovid, trazodone) and electrolyte loss in the setting of nausea, vomiting, and poor intake. After resuscitation, she developed melena and epigastric pain. Initial EGD revealed circumferential necrosis of the distal esophagus. The stomach was fluid-filled with retained gastric contents, raising concern for a distal obstructive process. NG decompression was deferred initially due to mucosal fragility. Abdominal CT showed a massively distended stomach with proximal duodenal obstruction. Repeat EGD demonstrated a duodenal ulcer and a tight, impassable narrowing in the second portion of the duodenum. Exploratory laparotomy revealed dense fibrotic tissue encasing the duodenum and biliary tree. She underwent Roux-en-Y gastrojejunostomy and choledochojejunostomy. Postoperatively, she recovered well on parenteral nutrition and high-dose proton pump inhibitors, and follow-up endoscopy showed esophageal healing. Discussion: Though RPF rarely affects the GI tract, it may cause critical complications through extrinsic compression and ischemia. Duodenal obstruction likely resulted from extrinsic compression by fibrotic tissue, while upstream gastric distention and reflux likely contributed to ischemic mucosal injury and acute esophageal necrosis. The patient’s torsades and cardiac arrest may have precipitated low-flow states, further exacerbating mucosal vulnerability. AEN is a rare manifestation of mucosal ischemia that demands early recognition. Although steroids may reverse early RPF changes, extensive fibrosis mandates surgical bypass. Early recognition of multisystem involvement is essential for preventing life-threatening complications and guiding multidisciplinary care.
Figure: Figure 1: A) Endoscopic image showing black necrotic mucosa of the distal esophagus (AEN). B) CT showing a distended stomach with transition point at the second portion of the duodenum.
Disclosures: Ishan Antony indicated no relevant financial relationships. Vian Rifat indicated no relevant financial relationships. Narinderjeet Kaur indicated no relevant financial relationships. Yasmine Agha indicated no relevant financial relationships.
Ishan Antony, MD1, Vian Rifat, MBBCh2, Narinderjeet Kaur, MD, MS3, Yasmine Agha, MD4. P5025 - Retroperitoneal Fibrosis Presenting With Black Esophagus and Gastric Outlet Obstruction: A Multisystem Complication of a Rare Fibrosing Disorder, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.