P5021 - Bronchoesophageal Fistula Formation Following Radiation and Lenvatinib Treatment for Hepatocellular Carcinoma After Recent Gastrostomy Tube Placement
Lenox Hill Hospital, Northwell Health New York, NY
Neil Gambhir, DO, Chun Lam, DO, Jordan Kazakov, MD Lenox Hill Hospital, Northwell Health, New York, NY Introduction: Bronchoesophageal fistulas (BEFs) are an aberrant connection formed between a major bronchus and the esophagus. A majority of BEFs in adults are acquired as a complication of trauma, iatrogenic intervention, infection, or malignancy and carry a high mortality risk. We describe the case of a 61-year-old woman with history of metastatic hepatocellular carcinoma to the lungs, treated with radiation and immunotherapy with Lenvatinib found to have a BEF. We hope that this report can serve to bring awareness to these unusual fistulas.
Case Description/
Methods: The patient is a 61-year-old female with a history of metastatic hepatocellular carcinoma (on Lenvatinib and steroids), diabetes, and GERD presented with 1-week history of SOB, abdominal pain, and fever. She had undergone PEG tube placement at an outside hospital one week prior.
On admission, vitals were significant for T 102.8°F, HR 126, BP 90/50 post 2.4L NS and SpO2 95% on 6L NC. On physical exam the patient had a positive Onos sign, coarse breath sounds, and erythematous PEG site. Chest X-ray demonstrated a left upper lobe and middle lobe opacities. Chest CT revealed subcutaneous abdominal gas with inflammation, new multifocal pulmonary opacities, a left perihilar consolidation, and multiple hepatic lesions. The patient was admitted to the medical ICU and was started on broad spectrum antibiotics.
On hospital day 4, the patient decompensated, continued to have fevers and worsening respiratory distress and subsequently intubated. Post-intubation she was noted to have abdominal distension which was relieved via PEG venting and large ventilator air leak noted. Emergent bronchoscopy revealed a BEF in the left mainstem bronchus ~1 cm above the secondary carina; endoscopy confirmed a 5 cm fistula distal to the incisors that was not previously present [Fig 1.]. A fully covered metal stent was placed across the fistula for palliation, and the patient was successfully extubated. Retrospective CT review showed bronchial-esophageal communication [Fig 2]. Unfortunately, on day 13, she developed acute hemoptysis and passed from cardiac arrest. Discussion: BEFs, though rare confer a high degree of mortality with chemotherapy and immunotherapy being linked to fistula formation. Nevertheless, our patient had multiple risk factors, including prior radiation, diabetes, and chronic steroid use, all impairing wound healing. Patients with these risks should be closely monitored for BEF development
Figure: Fig 1: Bronchoesophageal fistual (BEF) 1 cm above the left secondary carina demonstrated on bronchoscopy
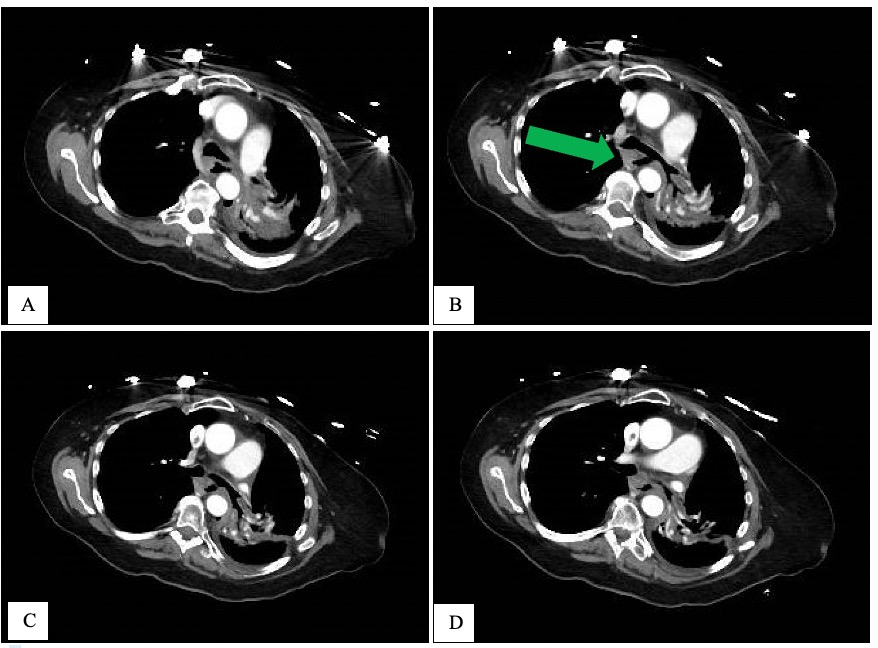
Figure: Fig 2: Retrospective CT review of the abdomen and chest on admission revealed a fistula between the left main bronchus and esophagus
Disclosures: Neil Gambhir indicated no relevant financial relationships. Chun Lam indicated no relevant financial relationships. Jordan Kazakov indicated no relevant financial relationships.
Neil Gambhir, DO, Chun Lam, DO, Jordan Kazakov, MD. P5021 - Bronchoesophageal Fistula Formation Following Radiation and Lenvatinib Treatment for Hepatocellular Carcinoma After Recent Gastrostomy Tube Placement, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.