Ivana Rubenstein, DO1, Andrea Escalante, DO2, Alexander Ting, DO1, Bianca Vahia, DO1, Alexa Torcini, DO1, Lloyd Bijuli-Singh, MD1, Hootan Vakili, MD3, Satya Singh, MD1 1Broward Health Medical Center, Fort Lauderdale, FL; 2Broward Health Medical Center, Miami, FL; 3Broward Health North, Pompano Beach, FL Introduction: Primary mediastinal germ cell tumors (PMGCTs) are rare extragonadal neoplasms, typically affecting young males. Yolk sac tumors are a malignant subtype characterized by elevated alpha-fetoprotein (AFP) and aggressive local invasion. Involvement of the esophagus is exceptionally rare and often leads to delayed diagnosis due to nonspecific symptoms.
Case Description/
Methods: A 34-year-old male with no known medical history who presented with a 3-month history of worsening cough, shortness of breath, vomiting, and fatigue. He reported episodes of hematemesis and was unable to tolerate oral intake. CTA chest revealed a large middle mediastinal and subcarinal lesion containing internal air, concerning for malignancy with potential esophageal communication or superimposed infection. Additional findings included right lower lobe aspiration pneumonia and extensive mediastinal, hilar, and intra-abdominal lymphadenopathy.
Upper endoscopy identified a 90 mm fungating, ulcerated esophageal mass in the middle third of the esophagus. Cold forceps biopsy demonstrated a malignant epithelioid neoplasm with abundant inflammatory stroma. Immunohistochemistry was positive for CDX2, SALL4, CD117, AFP, glypican-3, and strong pankeratin expression—findings consistent with a yolk sac tumor. The tumor was negative for CK7, CK20, TTF1, CD30, OCT4, and PLAP. AFP was significantly elevated at 797.86 ng/mL; beta-HCG was negative. Further imaging with CT abdomen/pelvis revealed calcified and hyperdense periaortic and portacaval lymphadenopathy. MRI brain and a nuclear medicine bone scan were negative for metastasis. Liver biopsy was deferred. The pathology and clinical features were consistent with a primary mediastinal yolk sac tumor involving the esophagus. Discussion: This case highlights a rare presentation of a primary mediastinal yolk sac tumor with direct esophageal invasion, presenting with hematemesis, dysphagia, and aspiration pneumonia. The diagnosis was supported by elevated AFP and characteristic immunophenotyping. Primary mediastinal yolk sac tumors can present with atypical gastrointestinal symptoms due to local invasion. Clinicians should maintain a high index of suspicion in young males with mediastinal masses and elevated AFP. Prompt biopsy and oncologic evaluation are essential for diagnosis and treatment planning, which typically involves neoadjuvant chemoradiation followed by surgery. Given the rarity and aggressive nature of these tumors, early recognition and a multidisciplinary approach are critical.
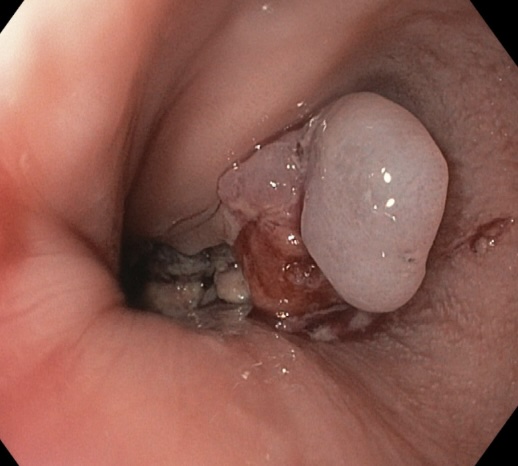
Figure: Figure 1: Endoscopic image showing a single fungating, invasive, and ulcerated mass measuring 90 mm in the middle third of the esophagus.
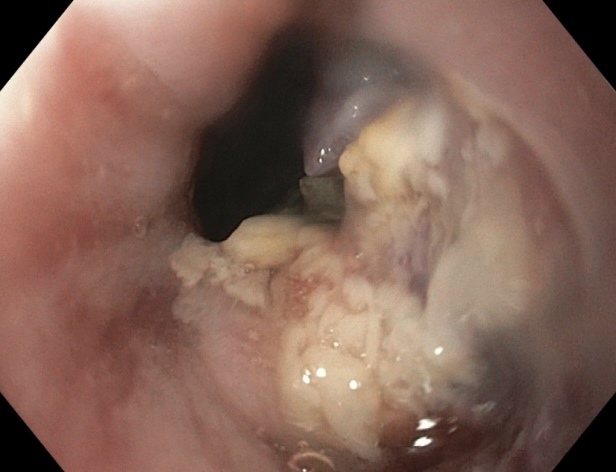
Figure: Figure 2: "Endoscopic view of a 90 mm fungating, invasive, and ulcerated mass in the middle third of the esophagus, following partial resection and biopsy.
Disclosures: Ivana Rubenstein indicated no relevant financial relationships. Andrea Escalante indicated no relevant financial relationships. Alexander Ting indicated no relevant financial relationships. Bianca Vahia indicated no relevant financial relationships. Alexa Torcini indicated no relevant financial relationships. Lloyd Bijuli-Singh indicated no relevant financial relationships. Hootan Vakili indicated no relevant financial relationships. Satya Singh indicated no relevant financial relationships.
Ivana Rubenstein, DO1, Andrea Escalante, DO2, Alexander Ting, DO1, Bianca Vahia, DO1, Alexa Torcini, DO1, Lloyd Bijuli-Singh, MD1, Hootan Vakili, MD3, Satya Singh, MD1. P5018 - Primary Mediastinal Yolk Sac Tumor: A Rare Cause of Esophageal Invasion and Gastrointestinal Symptoms in a Young Male, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")