University of Texas Health San Antonio San Antonio, TX
Mark Shokralla, DO1, Grecia Dominguez Rivera, MD1, Andrew Han, MD2 1University of Texas Health San Antonio, San Antonio, TX; 2South Texas Veterans Health, San Antonio, TX Introduction: Inlet patches (IPs) are areas of heterotopic gastric mucosa, usually located just below the upper esophageal sphincter and often discovered incidentally during endoscopy. While most IPs are focal and asymptomatic, fully circumferential inlet patches (FCIPs) are rare but often cause symptoms such as dysphagia, chronic cough, and globus sensation due to acid secretion and mucosal irritation.
Case Description/
Methods: A 67-year-old obese male veteran with a medical history of hyperlipidemia, hypothyroidism, and chronic obstructive pulmonary disease (COPD) presented for follow-up evaluation of longstanding gastroesophageal reflux disease (GERD) and dysphagia. He reported experiencing reflux symptoms for over five years, initially managed by his primary care provider with a proton pump inhibitor (PPI), which led to symptom improvement within 4 months.
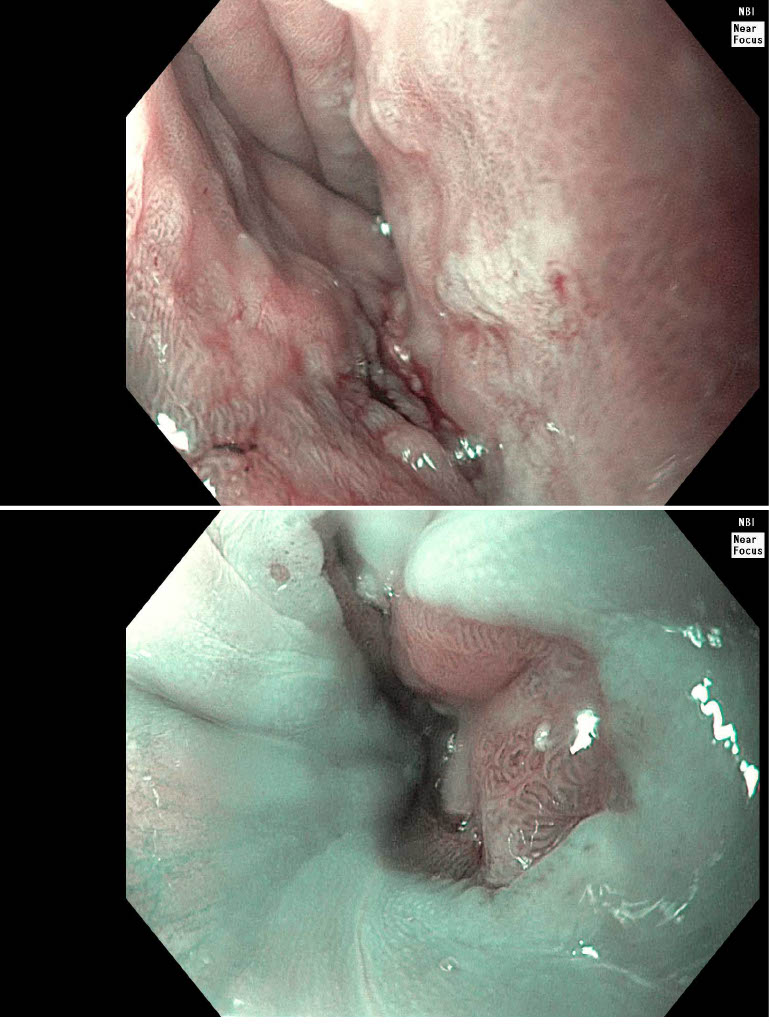
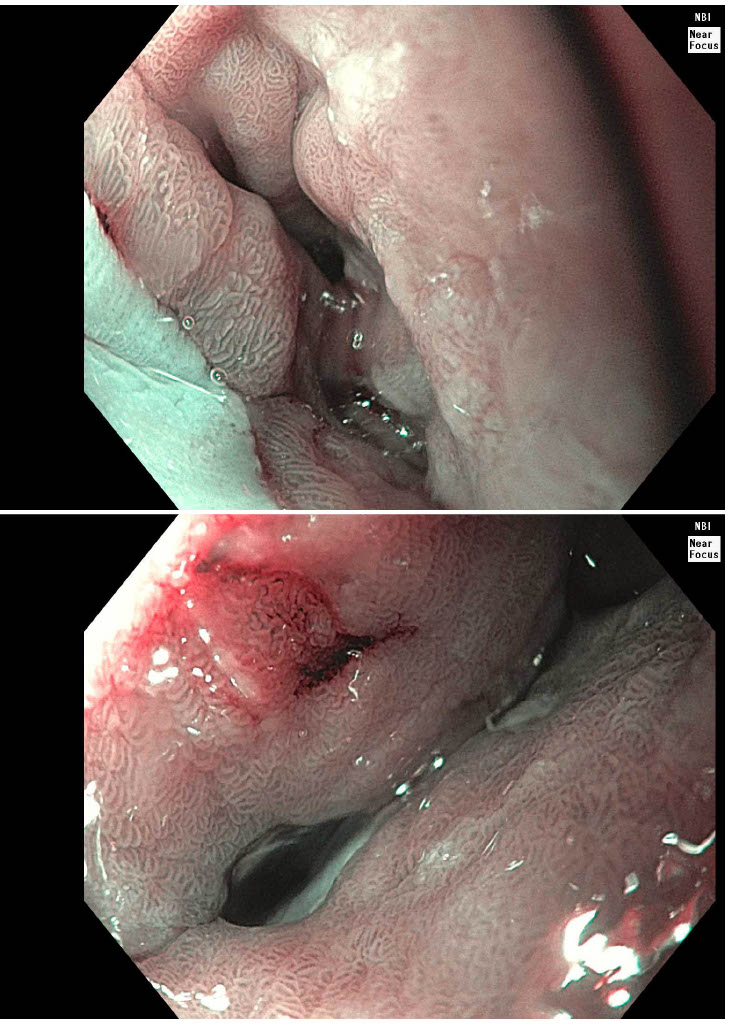
In 2019, he was referred to a community gastroenterologist due to persistent symptoms. An esophagogastroduodenoscopy (EGD) at that time revealed a 2–3 cm circumferential inlet patch located in the proximal esophagus. Biopsies confirmed heterotopic gastric oxyntic mucosa without evidence of metaplasia, dysplasia, or malignancy. He continued medical therapy with symptom control. In 2024, the patient re-established care and he reported ongoing intermittent dysphagia to solid foods and occasional coughing, but no difficulty with liquids. He had adopted lifestyle modifications, including smaller bites, thorough chewing, and dietary adjustments. A repeat EGD revealed a large, fully circumferential inlet patch extending from 18 to 22 cm from the incisors, with a sharp transition from squamous to salmon-pink columnar mucosa consistent with gastric heterotopia. No ulceration, bleeding, or strictures were observed. Histopathology again demonstrated heterotopic gastric oxyntic mucosa.
Given adequate symptom control on PPI therapy, the patient was managed conservatively with continued acid suppression and lifestyle modifications. Discussion: FCIPs often produce significant symptoms and can lead to significant complications including strictures, ulcers, or even adenocarcinoma. Diagnosis relies on endoscopic and histologic evaluation. Management is typically conservative with anti-secretory medications; endoscopic therapy may be needed to treat complications. Although preneoplastic changes are rare, long-term PPI therapy is advised to prevent complications such as strictures. Further studies are needed to guide management of symptomatic, treatment-resistant FCIPs.
Figure: FCIP #1
Figure: FCIP #2
Disclosures: Mark Shokralla indicated no relevant financial relationships. Grecia Dominguez Rivera indicated no relevant financial relationships. Andrew Han indicated no relevant financial relationships.
Mark Shokralla, DO1, Grecia Dominguez Rivera, MD1, Andrew Han, MD2. P4980 - Dysphagia Secondary to Fully Circumferential Inlet Patch: A Case Report, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.