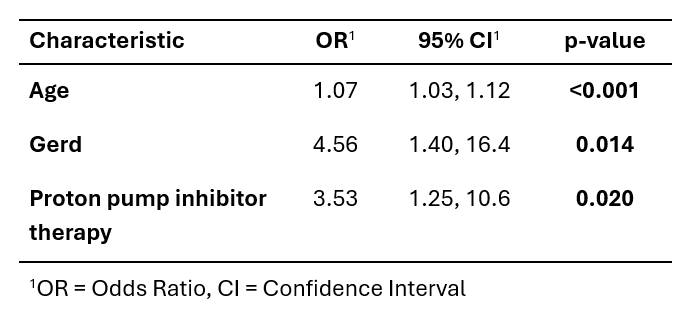
Claire Beveridge, MD1, Hussam Kawas, MD2, Qijun Yang, MS1, Andrei Ivanov, PhD1, Scott L. Gabbard, MD, FACG3, Florian Rieder, MD2 1Cleveland Clinic, Cleveland, OH; 2Cleveland Clinic Foundation, Cleveland, OH; 3Cleveland Clinic Foundation, Shaker Heights, OH Introduction: Delayed diagnosis increases the risk of complications in eosinophilic esophagitis (EoE). Misidentification of EoE may play a role, but data is limited. The aim of this study was to assess the frequency of a missed EoE diagnosis as well as relevant predictors. Methods: We performed a retrospective study of adult EoE patients seen at our center between 12/2024 and 02/2025. We excluded patients with missing endoscopic and/or histologic data. EoE was defined as ≥15 peak eosinophils per high power field (eos/hpf) with known esophageal dysfunction and no other cause of eosinophilia. Charts (including outside hospital data) were reviewed for demographics, endoscopic findings, EoE endoscopic reference score (EREFS), eos/hpf, comorbidities, medications, and symptoms. Gastroesophageal reflux disease (GERD) was defined as LA grade B-D esophagitis, peptic stricture, Barrett’s esophagus, or acid exposure time of >6%. Missed EoE (mEoE) was defined as a patient receiving an endoscopic evaluation prior to being diagnosed with EoE. Analysis includes descriptive statistics and logistic regression. Results: Out of 99 patients who met the inclusion criteria, 38 (38.4%) were mEoE. 71.1% (n=27) underwent an endoscopy for dysphagia, heartburn or food impaction. 86.8% (n=33) lacked esophageal biopsies due to a normal appearing esophagus (n=31) or an active food bolus impaction (n=2). 13.2% (n=5) were biopsied with 2 patients having 0 eos/hpf while on proton pump inhibitor (PPI) therapy and 3 patients with ≥15 eos/hpf in only distal esophagus therefore not given an EoE diagnosis. Median time from mEoE to diagnosis was 5.98 years (IQR: 2.4-9.9). There was no significant difference between cohorts (mEoE and non-mEoE) in terms of sex, race, ethnicity, BMI, atopic comorbidities, history of food impaction, and presence of fibrostenosis. mEoE patients were more likely to be older at diagnosis (OR 1.07, 95% CI: 1.03-1.11, p< 0.001), have a concurrent diagnosis of GERD (OR 4.23, 95% CI 1.47-13.3, p=0.009), already be on PPI therapy at time of diagnosis (OR 2.66, 95% CI 1.08-6.71, p=0.034). This remained true in a multivariate regression model. (Table 1) Discussion: Many EoE patients had a missed diagnosis of nearly 6 years. This highlights the need for planned esophageal biopsies in all patients presenting with esophageal dysfunction. Concomitant GERD contributes to mEoE as endoscopists may not be assessing for additional causes of esophageal symptoms.
Claire Beveridge, MD1, Hussam Kawas, MD2, Qijun Yang, MS1, Andrei Ivanov, PhD1, Scott L. Gabbard, MD, FACG3, Florian Rieder, MD2. P4942 - Eosinophilic Esophagitis: How Often Is the Diagnosis Missed?, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.