
Tuesday Poster Session
Category: Endoscopy Video Forum
 photo")
Taylor Bowler, DO (she/her/hers)
University of Minnesota Medical Center
Minneapolis, MN
Endoscopic full thickness resection (EFTR) using the full thickness resection device (FTRD) is a safe and effective technique for management of subepithelial lesions (SEL). This technique utilizes a grasping forceps to facilitate retraction into the FTRD cap prior to clip deployment followed by resection using snare with electrocautery. However, this technique can be challenging with SELs since the grasping forceps often capture the mucosa only leading to slippage of the underlying SEL. This limitation can be overcome with initial mucosal incision and unroofing to expose the underlying lesion and allow for full thickness resection using the FTRD. In this case report, we outline the technique of EFTR using the FTRD after mucosal unroofing of a gastric SEL.
Case Description/
Methods:
A 65-year-old male with history notable for tobacco use and seizure disorder was referred for management of a gastric SEL. Endoscopic ultrasound (EUS) demonstrated a 11 mm x 5 mm hypoechoic lesion originating from the submucosa (layer III) of the gastric body. Prior fine needle biopsies were non diagnostic. Endoscopic exam with white light imaging showed a 11 mm SEL with negative pillow sign (Figure 1A). Initial mucosal incision was performed with an endoscopic submucosal dissection (ESD) knife to unroof the underlying lesion (Figure 1B). Exposure of the lesion beneath the mucosal surface allowed for direct grasping of the lesion with the grasping forceps, retraction into the FTRD cap, and subsequent full thickness resection using the FTRD. Full thickness resection was demonstrated by the fatty patch within the clip and the specimen was successfully retrieved (Figure 1C). Lesion histopathology showed pancreatic heterotopia involving the submucosa with focal mucosal erosion (Figure 1D). There were no adverse events associated with the procedure.
Discussion: Overall, this case highlights that mucosal unroofing can allow for successful EFTR for resection of SELs. Future studies are needed to explore the utility of this technique compared to traditional endoscopic resection methods for management of gastric SELs. 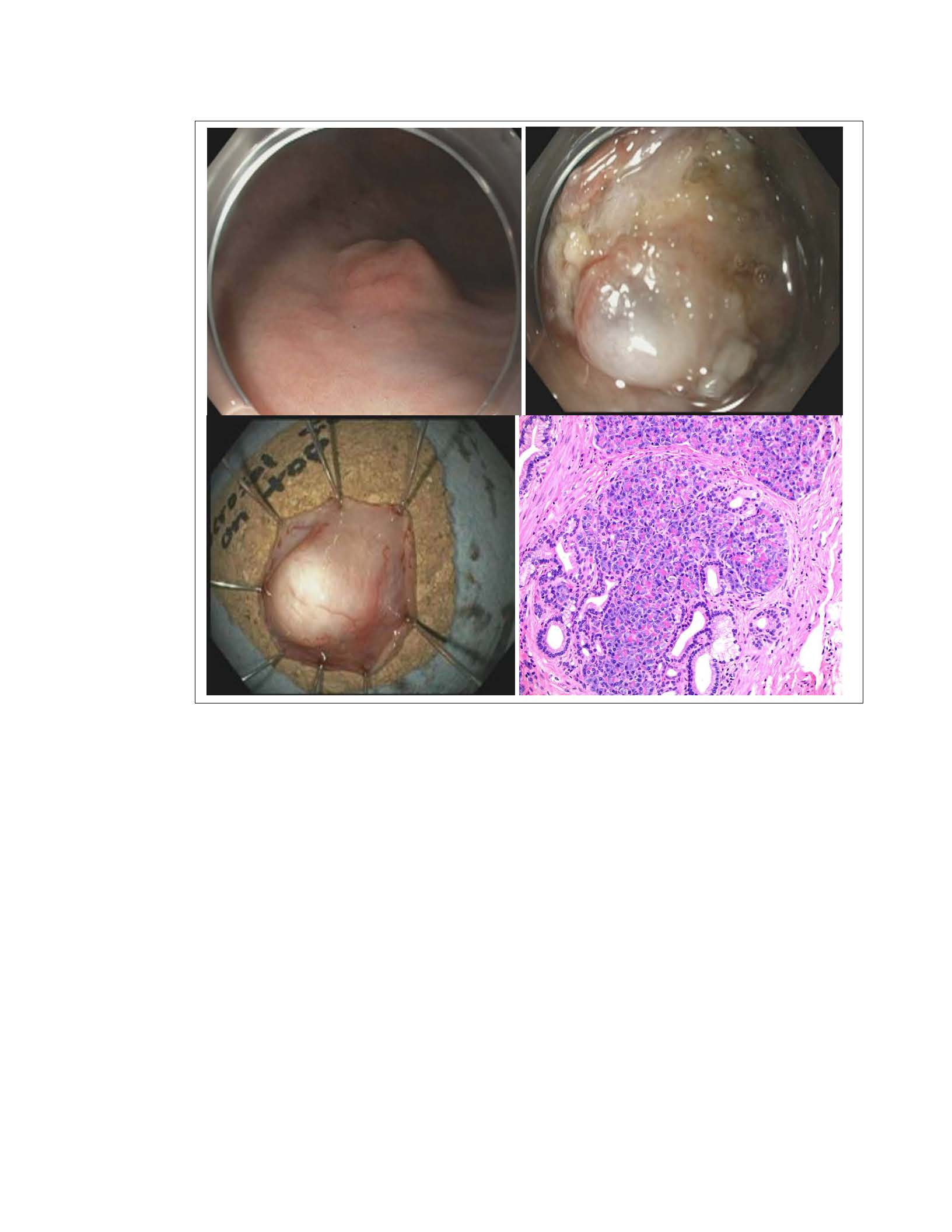
Figure: Figure 1A: SEL in gastric body. 1B: SEL after mucosal unroofing technique. 1C: Successful retrieval of lesion after EFTR. 1D: Lesion histopathology demonstrating pancreatic heterotropia.
Disclosures:
Taylor Bowler indicated no relevant financial relationships.
Rahul Karna indicated no relevant financial relationships.
Timothy Davie indicated no relevant financial relationships.
Carlos Iwamoto indicated no relevant financial relationships.
Mohammad Bilal: Boston Scientific – Consultant. Cook Endoscopy – Consultant. Steris Endoscopy – Consultant.
Taylor Bowler, DO1, Rahul Karna, MD1, Timothy Davie, MD1, Carlos Iwamoto, MD2, Mohammad Bilal, MD, FACG3. P4863 - Mucosal Incision-Assisted Unroofing Technique for Endoscopic Full Thickness Resection of a Gastric Subepithelial Lesion, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.