Kevin P. Shah, MD, Nithya Mahakala, BA, Sri Komanduri, MD, MS Northwestern Medicine, Chicago, IL Introduction: The Paris Classification system provides a standard methodology to classify the morphology of polyps and assess risk of malignancy and submucosal invasion. Herein, we describe the case of a patient referred to a large academic center for endoscopic mucosal resection (EMR) of a large Paris IIc polyp with an unforeseen anatomic barrier to resection.
Case Description/
Methods: A 71-year-old patient with family history of colorectal cancer and personal history of adenomatous polyps underwent surveillance colonoscopy at an outside hospital. During this procedure, a 3 cm granular polyp was identified in the sigmoid colon. Approximately half of the polyp was removed with underwater EMR using snare polypectomy, but due to technically challenging positioning and depression of the lesion into a fold, the procedure was aborted. Pathology revealed adenoma with villous features, and the patient was referred to a large academic center for expert attempt at resection.
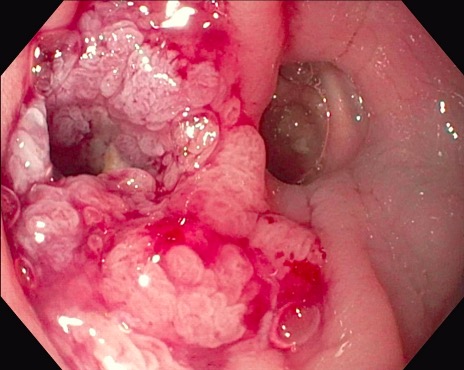
On repeat colonoscopy, the polyp was visualized at 45 cm from the anal verge. It measured approximately 30 mm in size and was noted to have Paris IIc morphology. Upon careful inspection and examination, the polyp was noted to be growing around and extending into a colonic diverticulum (Image 1). Attempts at submucosal injection were made using a sclerotherapy needle, but the lesion did not raise. Due to high perforation risk and inability to achieve R0 resection, the polyp was not amenable to an attempt at endoscopic resection. Tattoos were placed proximally and distally to the lesion and the patient was referred to colorectal surgery for definitive resection. Discussion: Typically, Paris IIc polyps greater than 20 mm in size should undergo en bloc resection with an experienced endoscopist, given high risk of submucosal invasion of the lesion. However, this case highlights an under-recognized challenge in the resection of a high-risk polyp: diverticular involvement of the lesion. Diverticula often have a markedly thin or absent muscularis propria layer, thereby placing patients at higher risk of complications of resection including full-thickness defects and perforation. This case underscores the importance of high-quality examination for lesion characterization, including but not limited to careful inspection, lifting, and the use of virtual chromoendoscopy. In such cases, multidisciplinary coordination between interventional endoscopy and colorectal surgery is critical to ensure a safe patient outcome.
Figure: This image shows a Paris IIc polyp that is growing around and extending into a diverticulum.
Disclosures: Kevin Shah indicated no relevant financial relationships. Nithya Mahakala indicated no relevant financial relationships. Sri Komanduri indicated no relevant financial relationships.
Kevin P. Shah, MD, Nithya Mahakala, BA, Sri Komanduri, MD, MS. P4819 - An Unforeseen Barrier to Endoscopic Mucosal Resection (EMR) of a Complex Polyp, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Kevin P. Shah, MD photo")