McKenna Andrews, MD1, Hezborn Magacha, MD2, Paul Robert Scott, 2, Jason Mckinney, MD2, James Denham, MD2 1East Tennessee State University, Kingsport, TN; 2East Tennessee State University, Johnson City, TN Introduction: Endometrial carcinoma is a common cancer in women, typically diagnosed around age 61. It often remains uterine-confined but can metastasize to lymph nodes, lungs, liver, and bones. Rectal metastasis is rare and may mimic primary colorectal disease, highlighting the need for broad differentials in postmenopausal women with rectal symptoms.
Case Description/
Methods: A 62-year-old woman with hypertension, hyperlipidemia, allergic rhinitis, and prior tobacco use presented with rectal pain and postmenopausal spotting. Symptoms included intermittent rectal discomfort, worsened by sitting, relieved by defecation, and bright red blood per rectum. Initially diagnosed with a rectal fissure and treated with diltiazem by primary care with her symptoms progressing to spasms and persistent bleeding. Patient was referred to colorectal surgery diagnosed with a chronic anal fissure, surgery was offered but declined, and nitroglycerin was started. Persistent spotting led to gynecologic referral. Ultrasound showed a thickened, hyper vascular endometrium (26.7 mm), and curettage confirmed FIGO grade 2 endometrioid adenocarcinoma. Pap smear and prior colonoscopy were unremarkable. On exam, a midline posterior rectal fissure was observed. Labs were normal. A CT scan revealed a heterogeneous rectal mass distinct from the uterine endometrium, raising suspicion for metastatic disease. Colonoscopy revealed diverticulosis, hemorrhoids, benign polyps, a fissure, and a rectal mass. Biopsy of the mass confirmed metastatic endometrioid adenocarcinoma. Immunostaining (CK7+, CK20-, CDX2-) supporting a gynecologic origin and verified by pathology. Discussion: This case illustrates a rare and diagnostically challenging presentation of metastatic endometrial cancer involving the rectum, initially resembling a chronic anal fissure. Rectal symptoms are an uncommon initial sign of endometrial carcinoma, often leading to misdiagnosis due to overlap with benign anorectal conditions. Absence of systemic findings or abnormal imaging further complicates early detection. Few such cases are reported in the literature. This case underscores the importance of including malignancy in the differential diagnosis of persistent anorectal symptoms in postmenopausal women, especially when accompanied by abnormal uterine bleeding, and highlights the value of multidisciplinary evaluation.
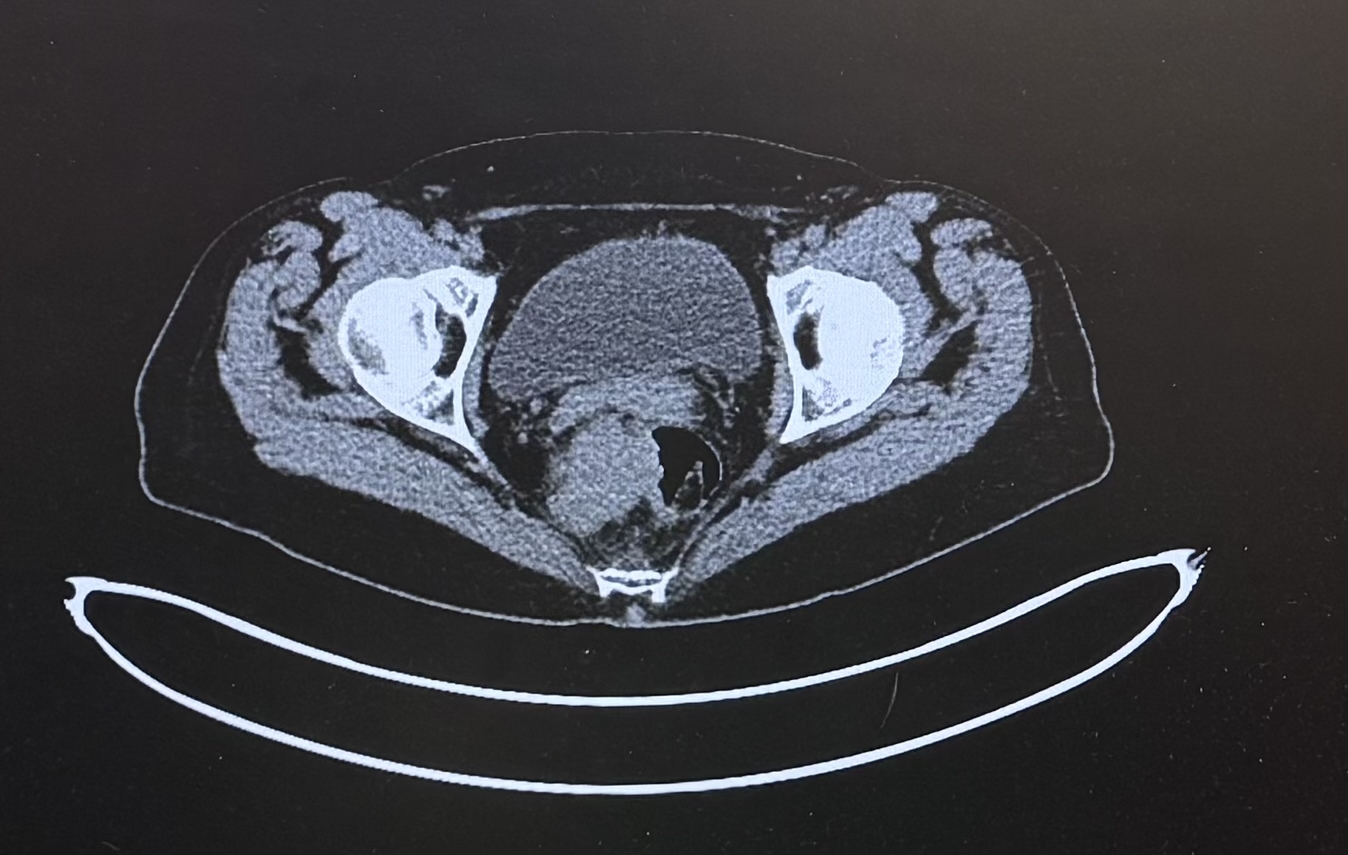
Figure: PET CT scan showing Hypermetabolism within the mass along the right lateral wall of the rectum, biopsy-proven metastatic disease.
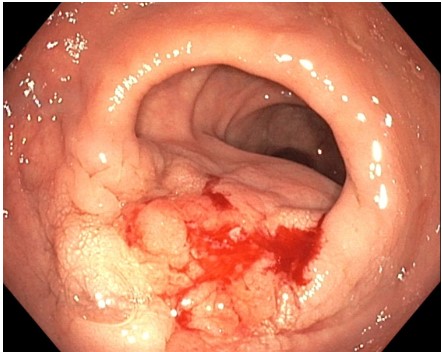
Figure: Rectal mass on Colonoscopy
Disclosures: McKenna Andrews indicated no relevant financial relationships. Hezborn Magacha indicated no relevant financial relationships. Paul Robert Scott indicated no relevant financial relationships. Jason Mckinney indicated no relevant financial relationships. James Denham indicated no relevant financial relationships.
McKenna Andrews, MD1, Hezborn Magacha, MD2, Paul Robert Scott, 2, Jason Mckinney, MD2, James Denham, MD2. P4814 - Metastatic Mislead: When Rectal Symptoms Reveal Endometrial Origin, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.