Hannah WF. Goodrich, MD1, Joao Monteiro, PhD2, Ross Hilliard, MD3, Ricky Grisson, MD4, Carrie Brdiges-Feliz, MPH5, Harlan G. Rich, MD6 1Yale Digestive Diseases, New Haven, CT; 2Brown University, Providence, RI; 3Maine Medical Center, Portland, ME; 4Brown Medicine/Lifespan, Providence, RI; 5Brown University / Rhode Island Hospital, Providence, RI; 6Brown Medicine/Brown Physicians, Inc., Providence, RI Introduction: One third of the eligible US population fails to undergo routine CRC screening. ACG’s Clinical Guidelines suggest utilizing patient navigators to improve adherence. We have previously shown that navigators can significantly increase return rates for FIT, helping prioritize patients for diagnostic colonoscopies. The critical next step is ensuring that patients with positive FIT go on to complete colonoscopy. Methods: We conducted a retrospective analysis of patient adherence from referral to completion of colonoscopy after positive FIT. Our dataset included 7148 FIT kit orders between 01/2017–09/2024; a dedicated patient navigator was introduced in 01/2021 to support FIT kit return. We examined the impact of this intervention on subsequent colonoscopy completion. Descriptive analyses (via SAS version 9.4) were performed using chi-square, Fisher’s exact, and Student’s t-tests. A multivariable linear regression model was used to compare pre- and post-intervention. Models were adjusted for gender, age, race and language. Results: There were 289 positive FIT results; 147 post- and 142 pre-intervention. Following positive FIT, 94.5% of patients received a referral for colonoscopy, with an average of 22.3 days from positive FIT to referral; overall rate of colonoscopy completion within 6 months was 32.5% (no significant difference between groups for any of these metrics). However, time from referral to completion was significantly shorter post-intervention (160.7±178.4 vs. 360.7±577.0 days; p=0.0174). This reduction in wait time was even more pronounced in key subgroups (age 51-64: 146.4±134.1 vs. 370.1±597.2, p=0.0481; White/Caucasian: 124.4±84.7 vs. 461.1±653.9, p=0.015; Medicare: 113.1±93.0 vs. 340.6±489.9, p=0.0330; English-speaking: 172.8±205.6 vs. 480.9±661.5, p=0.0152). Discussion: We explored longitudinal adherence to CRC screening via colonoscopy after the original intervention of patient navigator to support FIT kit return. Time from colonoscopy referral to completion was significantly shorter post-intervention. This improvement was likely two-fold: (1) With our intervention our schedulers became more attentive to positive FIT referrals; they in turn altered their IT scheduling support tools to focus on getting these patients scheduled in a timely manner. (2) Patients, due to prior navigation efforts, may have better understood the importance of a positive result and were thus more motivated to complete colonoscopy.
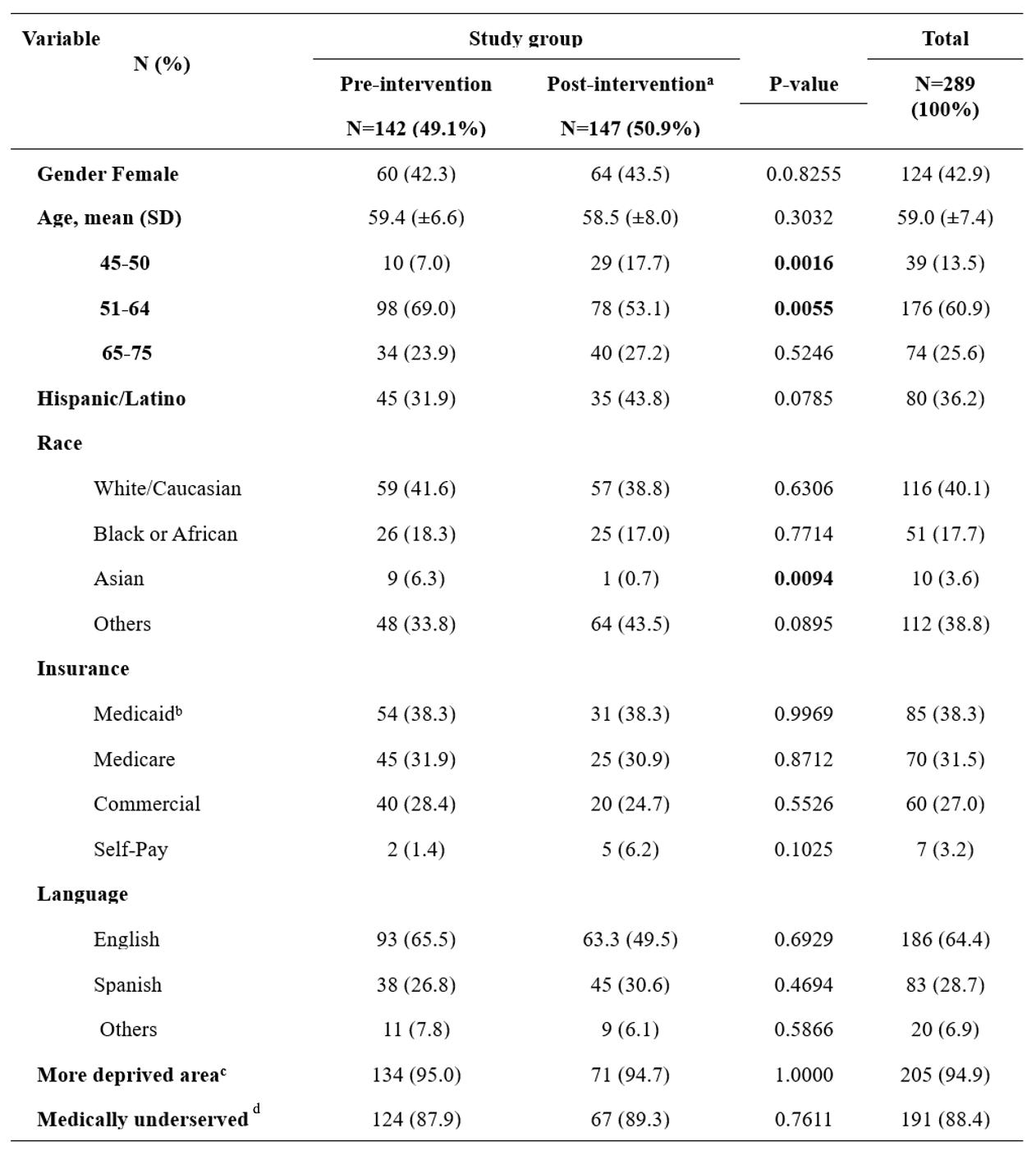
Figure: Figure 1: Baseline characteristics of patients who had an order for a FIT kit, comparing pre- and post-intervention periods, from 01/2017–09/2024.
Notes: (a) Starting in 01/2021 an intervention program was developed with the addition of a dedicated patient navigator to support patients in completing and returning their testing. (b) Also includes a state-based Medicaid health plan. (c) According to rankings of socioeconomic disadvantage. (d) Geographic areas/populations with poor access to primary health care services.
Abbreviations: FIT – fecal immunochemical test; SD – standard deviation.
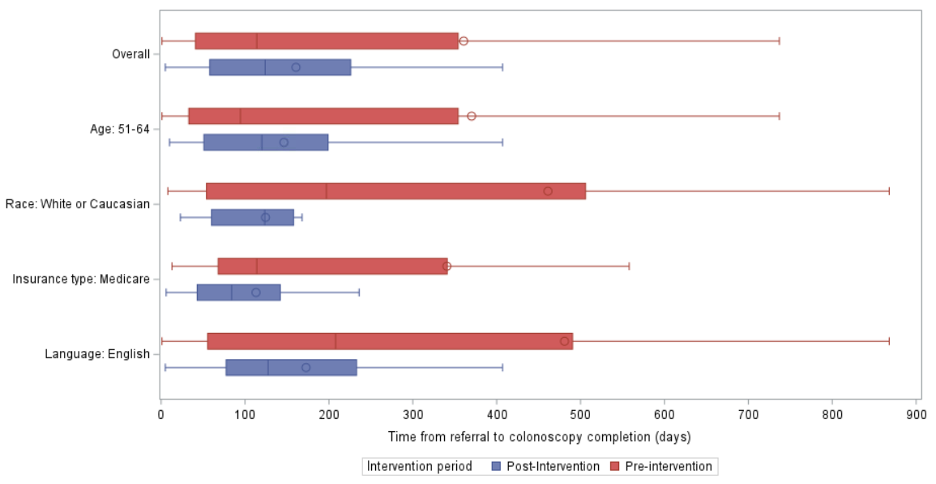
Figure: Figure 2: Time from referral for colonoscopy to completion of colonoscopy.
The time from referral to colonoscopy completion was significantly shorter in the post-intervention group (160.7 ± 178.4 days) compared to the pre-intervention group (360.7 ± 577.0 days), with an adjusted p-value of 0.0174.
This reduction in wait time was even more pronounced in key subgroups: (a) Individuals aged 51–64 years: average time decreased from 370.1 ± 597.2 days pre-intervention to 146.4 ± 134.1 days post-intervention (adjusted p=0.0481). (b) White/Caucasian patients: average time decreased from 461.1 ± 653.9 to 124.4 ± 84.7 days (adjusted p=0.0150). (c) Patients with Medicare coverage: average time decreased from 340.6 ± 489.9 to 113.1 ± 93.0 days (p=0.0330). (d) English-speaking patients: average time decreased from 480.9 ± 661.5 to 172.8 ± 205.6 days (adjusted p=0.0152).
Disclosures: Hannah Goodrich indicated no relevant financial relationships. Joao Monteiro indicated no relevant financial relationships. Ross Hilliard indicated no relevant financial relationships. Ricky Grisson indicated no relevant financial relationships. Carrie Brdiges-Feliz indicated no relevant financial relationships. Harlan Rich indicated no relevant financial relationships.
Hannah WF. Goodrich, MD1, Joao Monteiro, PhD2, Ross Hilliard, MD3, Ricky Grisson, MD4, Carrie Brdiges-Feliz, MPH5, Harlan G. Rich, MD6. P4774 - From Screening to Diagnosis: The Impact of Patient Navigation Services on Timely Colonoscopy After Positive Fecal Immunochemical Test, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")