George Washington University School of Medicine and Health Sciences Washington, DC
Maxwell S. Madani, BA1, Athanasios S. Naum, BS1, Robert S.. Gordon, DO, MS2, Omar K. Abu-Ghannam, BS1, Marie L. Borum, MD, EdD, MPH, FACG3 1George Washington University School of Medicine and Health Sciences, Washington, DC; 2George Washington University School of Medicine and Health Sciences, Arlington, WA; 3Division of Gastroenterology and Liver Disease, Department of Medicine, George Washington University School of Medicine and Health Sciences, Washington, DC Introduction: The incidence of anal squamous cell carcinoma (ASCC) has been increasing in the last two decades, at rates as high as 2.7% annually for those older than 50. This increase has been attributed to multiple factors including human papillomavirus (HPV), smoking, and immunosuppression. ASCC is an aggressive malignancy with a 3-year recurrence rate of up to 23%.3 The majority of reoccurrences present within 3 years of initial diagnosis (88%) with the liver (48%) and the lungs (10%) the most common sites for distant metastasis. We present a rare case of ASCC pulmonary recurrence 9 years following complete clinical response to treatment. This is the longest reported latency period between treatment and metastatic disease without locoregional manifestation.
Case Description/
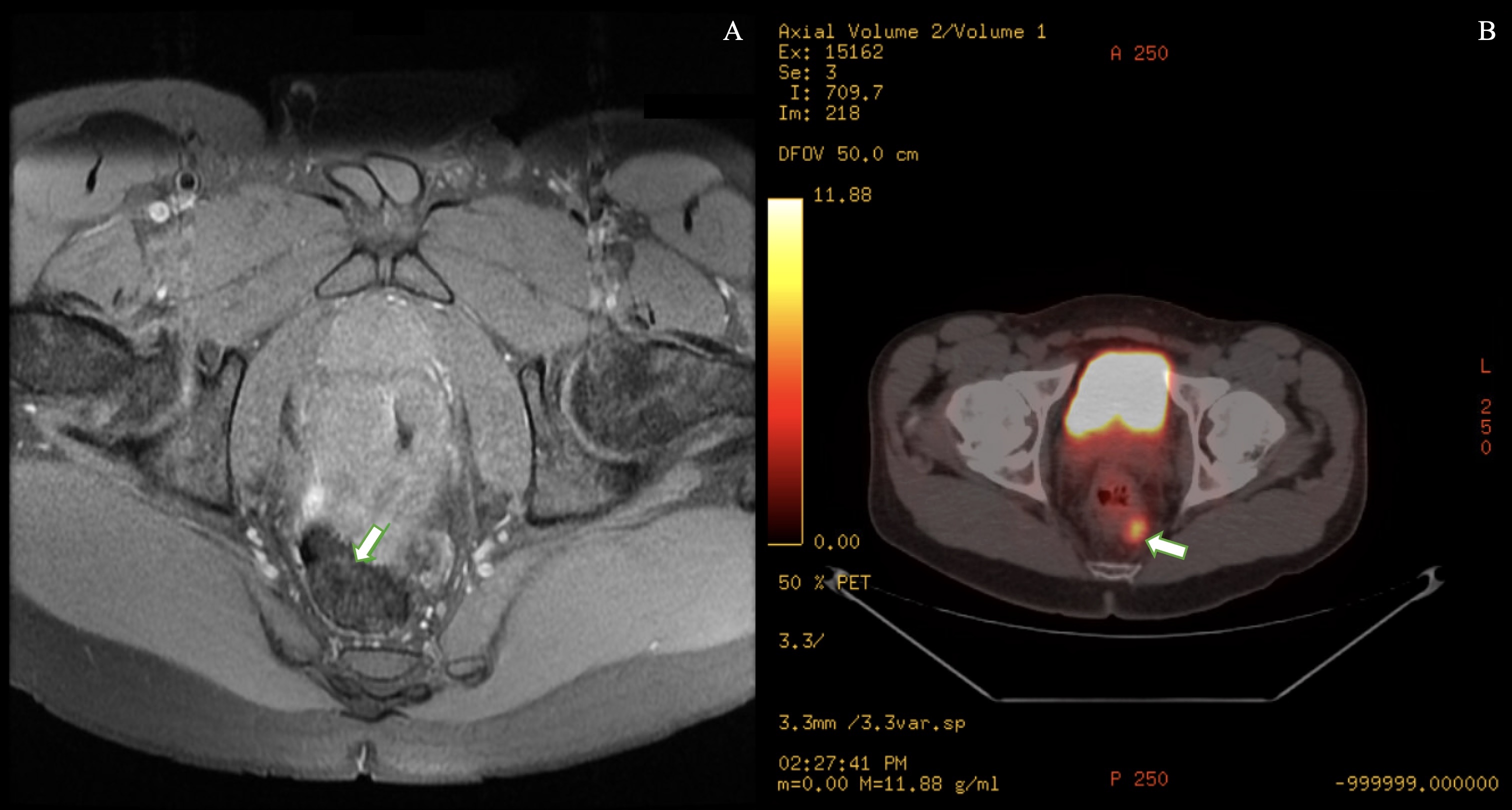
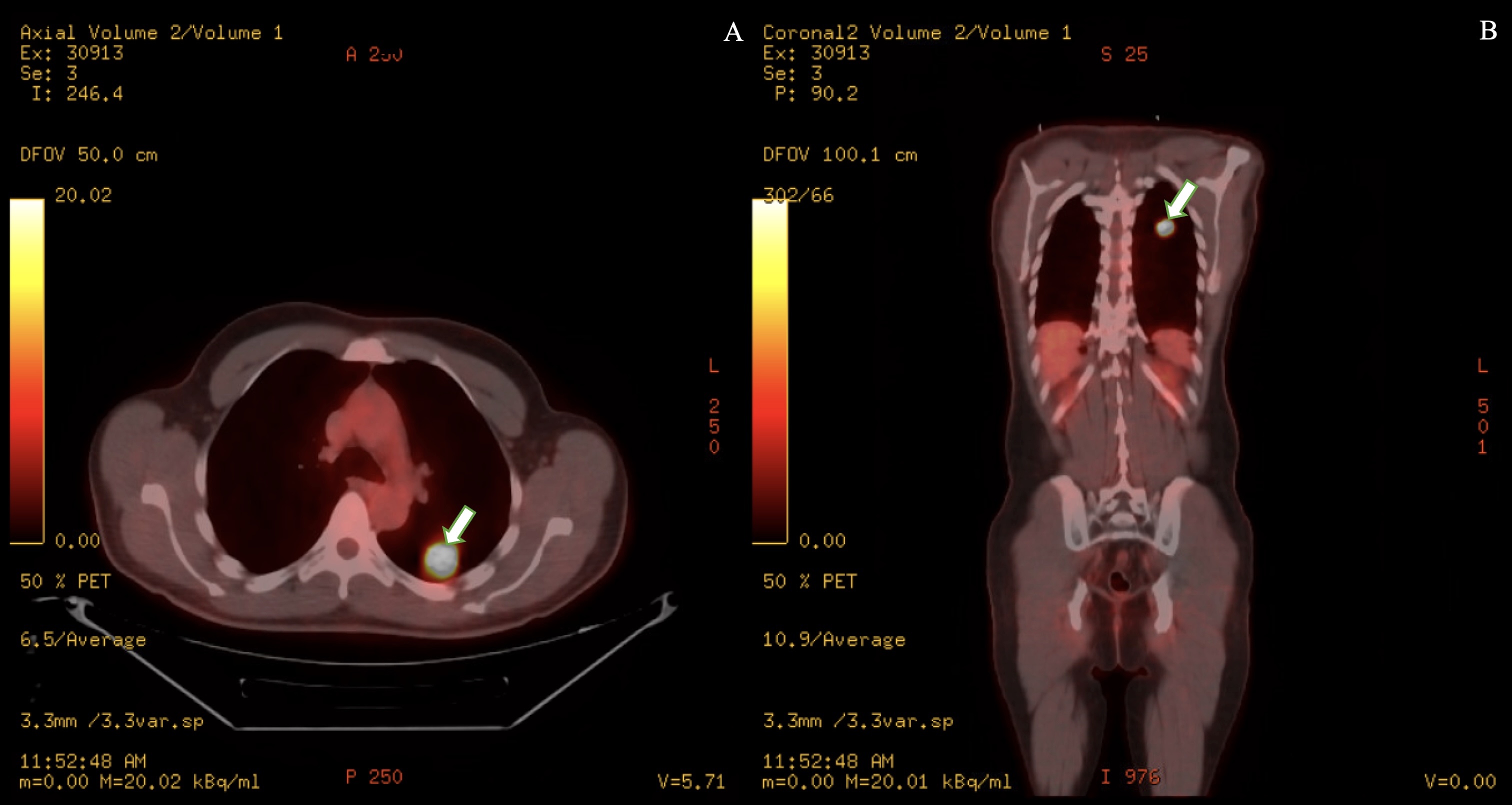
Methods: A 51-year-old male with history of HIV (CD4 512) with inconsistent highly active antiretroviral therapy (HAART) and anal squamous cell carcinoma (Figure 1) treated with radiation and chemotherapy 9 years prior who presented with 4 days of night sweats, chills, chest pain, abdominal pain, hematochezia and weight loss. His exam revealed tenderness to palpation in bilateral upper abdominal quadrants, but was otherwise unremarkable. A CT angiography of chest abdomen pelvis revealed a 2.7cm solid pulmonary nodule with features suspicious for a primary lung neoplasm. A CT-guided lung biopsy revealed squamous cell carcinoma that is positive for P40 and P16 consistent with HPV-associated diagnosis of SCC of anal/rectal origin. A PET/CT showed a max SUV of 17.2 for the left lower lobe pulmonary nodule, otherwise unremarkable for hypermetabolic activity (Figure 2). Subsequent colonoscopy, performed to further assess for locoregional recurrence, revealed only two ascending colon tubular adenomas and a rectal hyperplastic polyp. Discussion: Given that most ASCC recurrences occur in the first 3 years, this case is a remarkable deviation from the usual disease course. Additionally, this is the only documented case of late distant metastatic recurrence without any locoregional manifestations. It is important that there is recognition that immunosuppressed individuals can have unique displays of tumor recurrence. The use of HAART has been associated with a higher rate of relapse in HIV-positive patients. The patient’s inconsistent antiretroviral use may have contributed to the delayed presentation of the distant recurrence.
Figure: Figure 1A) 1.7 cm enhancing soft tissue lesion in the left supralevator space adjacent to the rectosigmoid junction. Figure 1B) 1.8 cm hypermetabolic left perirectal lymph node (Max SUV = 7.6).
Figure: Figure 2) Hyperbolic left lower lobe lung nodule with maximum SUV of 17.2; 2A) Axial view 2B) Coronal View.
Disclosures: Maxwell Madani indicated no relevant financial relationships. Athanasios Naum indicated no relevant financial relationships. Robert Gordon indicated no relevant financial relationships. Omar Abu-Ghannam indicated no relevant financial relationships. Marie Borum indicated no relevant financial relationships.
Maxwell S. Madani, BA1, Athanasios S. Naum, BS1, Robert S.. Gordon, DO, MS2, Omar K. Abu-Ghannam, BS1, Marie L. Borum, MD, EdD, MPH, FACG3. P4739 - Pulmonary Recurrence of Anal Squamous Cell Carcinoma 9 Years Following Treatment, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")