Tuesday Poster Session
Category: Colon
Zainab Saeed, MD (she/her/hers)
Houston Methodist Hospital
Houston, TX
A 63-year-old lady with a past medical history of type II diabetes mellitus, hyperlipidemia, and diverticulosis presented with chief complaint of two weeks of worsening abdominal pain associated with nausea and vomiting. The patient reported being on Semaglutide for the past 4 months, starting at 0.25mg weekly and currently at 1.7mg weekly.
She reported constipation since starting this medication, with bowel movements occurring once every 4-5 days. However, for the last 4 weeks, she has not had any bowel movements. However, she was able to pass flatus.
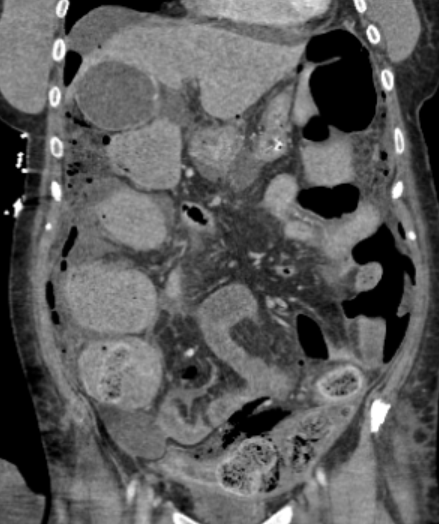
On admission, the patient was tachycardiac and hypotensive, with an elevated white blood cell count and lactic acidosis. Physical examination revealed a distended abdomen with absent bowel sounds. A CT scan of the abdomen showed colonic perforation with extravasation of stool, pneumoperitoneum, peritoneal wall thickening, and a large volume of stool burden throughout the entire colon.
The patient underwent an exploratory laparotomy, sigmoid colon resection due to distal mid colon perforation, with Hartmann’s pouch and colostomy creation. Attempts to milk out hard stool intraoperatively were unsuccessful as it caused further mucosal damage to the remaining colon. Patient remained on broad spectrum antibiotics while in hospital and later required IR guided drain placement for intra-abdominal loculated fluid collections. Patient was eventually discharged home.