University of Tennessee Health Science Center Bartlett, TN
Trenton Judd, DO1, Tyson Amundsen, MD2, Satheesh Nair, MD3 1University of Tennessee Health Science Center, Bartlett, TN; 2UTHSC, Memphis, TN; 3Methodist LeBonheur Healthcare, Memphis, TN Introduction: Colorectal cancer is among the most common malignancies globally, typically presenting as a primary cancer, with intracolonic metastases rare. Breast cancer seldom metastasizes to the GI tract, but when it does, it favors the stomach and small bowel. We present a rare case of breast cancer metastasizing to the colon, approximately five years after mastectomy and targeted hormonal therapy. The patient's care was complicated by her visiting status from another country, lack of insurance, and noncitizen designation.
Case Description/
Methods: A 66-year-old woman with a history of breast cancer and diabetes mellitus (managed with oral medications) presented with abdominal pain while visiting the U.S. from another country. She had previously undergone a unilateral mastectomy with hormonal therapy (palbociclib and fulvestrant). Her abdominal pain had persisted for weeks and was intermittent, cramping, and associated with nausea and vomiting. She denied weight loss, GI bleeding, or bowel habit changes. On evaluation, her vitals were normal, and labs showed mild anemia and elevated liver enzymes. CT revealed circumferential thickening of the transverse colon, suspicious for neoplasm. MRI showed a 7.1 cm lesion with enhancement and restricted diffusion, atypical for primary colon cancer and vertebral lesions (T12, L2, L4-5) suggesting metastasis. A prior PET from her home country showed no colon involvement but suggested minimal osseous metastases. Colonoscopy revealed a non-obstructing circumferential mass, which was biopsied. Histopathology confirmed metastatic breast carcinoma (positive for CK7, GATA-3, ER; HER-2/neu negative). Management included surgical, medical oncology, and palliative care evaluation. Surgery wasn’t indicated due to lack of obstruction and limited benefit. Oncologic therapy was discussed but complicated by her uninsured, nonresident status. She was ultimately discharged to family in the U.S. and returned to her home country when stable. Discussion: Breast cancer, though prevalent, rarely metastasizes to the colon. Both invasive ductal and lobular carcinomas can do so via hematogenous, lymphatic, or surgical dissemination. Mechanism here was uncertain. Diagnosis was made through endoscopic biopsy; in some cases, additional tools like EUS-FNA or PET may be needed as accurate diagnosis is critical to guide therapy. CMBC is rare, and should be considered in colon lesions in patients with a breast cancer history.
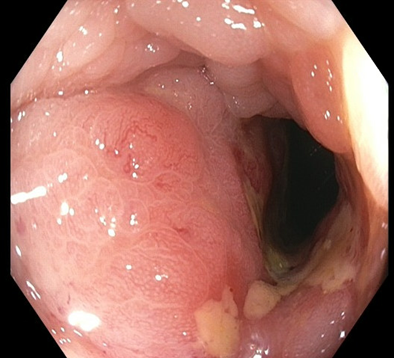
Figure: A non-obstructing circumferential colon mass seen in a case of CMBC.
Disclosures: Trenton Judd indicated no relevant financial relationships. Tyson Amundsen indicated no relevant financial relationships. Satheesh Nair indicated no relevant financial relationships.
Trenton Judd, DO1, Tyson Amundsen, MD2, Satheesh Nair, MD3. P4706 - Colonic Metastasis from Breast Cancer (CMBC): A Case or an Uncommon Disease With an Uncommon Scenario, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")