
Tuesday Poster Session
Category: Colon


 photo")
Samantha Vuong, BA (she/her/hers)
University of Wisconsin School of Medicine and Public Health, WI
Plasmacytoid urothelial carcinoma (PUC) is a rare, aggressive variant of urothelial carcinoma with a poor prognosis. Less than 20 cases of metastatic urothelial carcinoma presenting as a rectal stricture have been reported, with no known cases involving recurrent PUC.1,2 Here, we present a unique case of recurrent PUC presenting as a rectal stricture.
Case Description/
Methods:
A 57-year-old male with class III obesity, pilonidal cysts status-post incision and drainage with seton placement, and PUC (pT1N0M0) status-post radical cystoprostatectomy with ileal conduit 5 years prior presented with several months of rectal pain. Initial colonoscopy revealed rectal congestion, erythema, nodularity, and friability (Fig 1A). Histology showed patchy lamina propria fibrosis, vascular congestion and focal crypt withering suggestive of ischemic injury. Computed tomography (CT) angiogram showed patent vasculature. Magnetic resonance imaging (MRI) demonstrated extensive proctocolitis of the rectum and distal sigmoid colon with extensive inflammation throughout the pelvis, perirectal soft tissues, and pelvic musculature (Fig 1B). No autoimmune or infectious etiology was identified. The rectum was biopsied three other times without significant abnormality. Symptoms were refractory to steroids, antibiotics, and topical rectal therapies. He later presented to the emergency department with dizziness. CT abdomen revealed >20 cm of luminal narrowing in the distant sigmoid colon and rectum with proximal dilation concerning for partial obstruction (Fig 1C). Endoscopic decompression was attempted and aborted, as the severe stenosis impeded passage of the endoscope; distal biopsies showed rare malignant cells, too few to characterize. Subsequent imaging revealed worsening colonic dilation and pneumatosis and he underwent a diverting loop ileostomy. Further rectal biopsies were obtained, revealing recurrent PUC involving submucosal colonic tissue (Fig 1D, 1E).
Discussion:
This case presents a rare recurrence of PUC manifesting as rectal pain and proctitis with resulting high-grade anorectal stricture. The presentation posed a significant diagnostic challenge, with multidisciplinary evaluation and repeat biopsies failing to reveal the cause. PUC often presents at an advanced stage and can spread to peritoneal surfaces. Recurrent malignancy should be considered in patients with a history of PUC and undifferentiated gastrointestinal symptoms, especially in the absence of alternative etiology identified at symptom onset.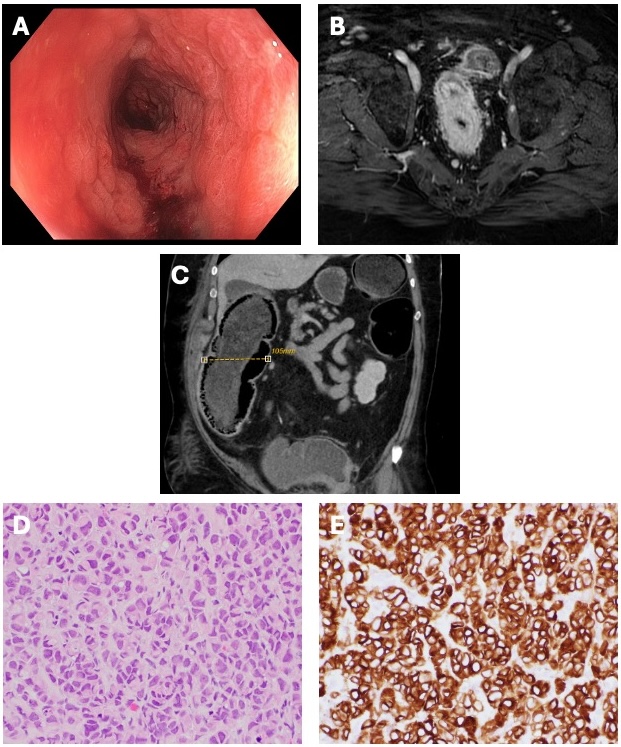
Figure: Figure 1: A. Colonoscopy revealing rectal inflammation characterized by congestion, erythema, nodularity, and friability. B. Extensive proctocolitis of the rectum seen on MRI. C. CT demonstrating partial large bowel obstruction, with right colon dilation to 10.5 cm. D. Hematoxylin-Eosin stain at x40 magnification shows single infiltrative malignant cells with eccentric nuclei, resembling plasma cells, which characterize the plasmacytoid variant of urothelial carcinoma. E. Immunostain for Uroplakin II demonstrates membranous expression in tumor cells confirming urothelial origin.
Disclosures:
Samantha Vuong indicated no relevant financial relationships.
Trevor Schell indicated no relevant financial relationships.
Saryn Doucette indicated no relevant financial relationships.
Christopher Lindholm indicated no relevant financial relationships.
Samantha Vuong, BA1, Trevor Schell, MD2, Saryn Doucette, MD2, Christopher Lindholm, MD2. P4684 - A Novel Case of Recurrent Metastatic Plasmacytoid Urothelial Carcinoma Presenting as a Rectal Stricture, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.