
Tuesday Poster Session
Category: Colon
 photo")
Mustafa V. Gecin, MD (he/him/his)
UPMC
Monroeville, PA
Solitary rectal ulcer syndrome (SRUS) is a rare, benign condition characterized by rectal bleeding, mucorrhea, and altered bowel habits, often linked to mucosal prolapse. Its endoscopic appearance may mimic malignancy. We present a 31-year-old man with iron deficiency anemia (IDA) and hematochezia, initially suspected to have rectal cancer, but ultimately diagnosed with SRUS in the setting of inflammatory cloacogenic polyps and pelvic floor dysfunction, along with eosinophilic esophagitis (EoE).
Case Description/
Methods:
The patient presented with IDA (ferritin 33 ng/mL, iron saturation 15%) and intermittent rectal bleeding. Colonoscopy on 9/27/2023 revealed multiple large ulcerated rectal nodules concerning for malignancy. Biopsies showed acute colitis without dysplasia or malignancy. Infectious workup was negative, including stains for CMV, HSV, and rectal swabs for STIs.
An EGD on 10/30/2023 for ongoing IDA showed EoE and multiple fundic gland polyps, likely PPI-related, without high-risk features. A follow-up EGD on 2/7/2024 revealed iron pill gastropathy, and oral iron was discontinued after IDA resolved.
Persistent anorectal symptoms and polypoid lesions prompted examination under anesthesia with transanal excision on 4/9/2024. Pathology revealed benign inflammatory cloacogenic polyps. In the context of mucosal prolapse, straining, and incomplete evacuation, the diagnosis of SRUS was made. IBD was considered but excluded due to absence of chronic inflammation or granulomas.
EoE was initially managed with PPIs, but repeat EGD on 5/1/2024 showed 62 eosinophils/hpf. Dupilumab was started on 5/22/2024. By July, dysphagia had resolved, and a follow-up EGD in November 2024 confirmed histologic remission.
By March 2025, the patient reported improvement in rectal symptoms with Benefiber but had not yet begun pelvic floor physical therapy. He remained on weekly dupilumab with sustained EoE remission and reported good symptom control. His most recent esophageal biopsies from November 2024 showed no intraepithelial eosinophils, consistent with histologic remission.
Discussion:
This case highlights the importance of considering SRUS and inflammatory cloacogenic polyps in the differential diagnosis of rectal masses in young patients presenting with IDA and prolapse-related symptoms. Multidisciplinary evaluation is critical. Early diagnosis can improve outcomes through targeted therapy, including dietary management, fiber supplementation, and pelvic floor rehabilitation.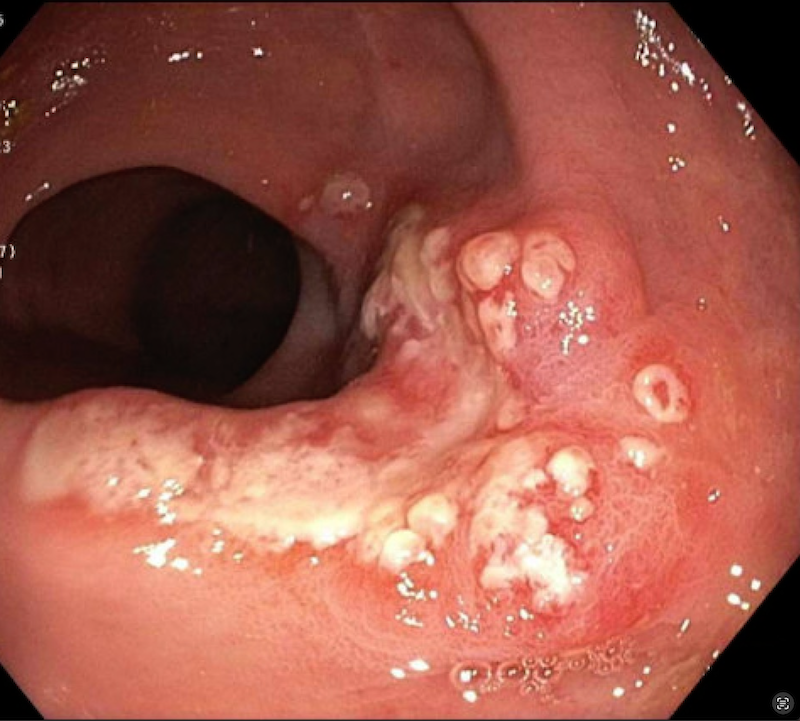
Figure: Nonbleeding ulcerated mucosa with no stigmata of recent bleeding were present in the rectum. Biopsies were taken with a cold forceps for histology.
Figure: A continuous area of nonbleeding ulcerated mucosa with no stigmata of recent bleeding was present at the anus. This was visible on direct endoscopic view on the anal canal as well as during retroflexion. Biopsies were
taken with a cold forceps for histology. Estimated blood loss was minimal.
Disclosures:
Mustafa Gecin indicated no relevant financial relationships.
Vladimir Lamm indicated no relevant financial relationships.
Mustafa V. Gecin, MD1, Vladimir Lamm, MD2. P4678 -
Case Report: Solitary Rectal Ulcer Syndrome Mimicking Malignancy With Concomitant Eosinophilic Esophagitis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.