
Tuesday Poster Session
Category: Colon

Adrianna Wierzbicka, MD
Cleveland Clinic Florida
Weston, FL
Rectovaginal endometriosis is a deceptive condition that can infiltrate the rectal wall and mimic gastrointestinal (GI) malignancy. Though endometriosis typically presents with pelvic pain and menstrual symptoms, it can occasionally manifest with isolated gastrointestinal symptoms. We present a case of a benign gynecologic disorder that convincingly presented as a rectal neoplasm with narrowing.
Case Description/
Methods:
A 45-year-old woman presented with several months of painless bright red rectal bleeding and chronic diarrhea. She denied any abdominal pain, dyschezia or weight loss. She reported a remote history of heavy menstrual bleeding, for which multiple transvaginal ultrasounds had previously been performed and were unremarkable. As part of the workup, a colonoscopy was performed which revealed a partially obstructing ulcerated mass in the mid-rectum (Figure 1). Biopsies demonstrated benign lymphoid nodule without evidence of malignancy. Despite this, the lesion’s endoscopic appearance raised concern for colorectal cancer.
Given the diagnostic uncertainty, further imaging was pursued for better lesion characterization. Contrast-enhanced pelvic MRI revealed a 5.8 cm spiculated soft tissue mass infiltrating the anterior rectal wall, contiguous with the posterior uterus, suggesting the possibility of deep infiltrating endometriosis (Figure 2). A multidisciplinary team proceeded with laparoscopic low anterior resection with en-block hysterectomy and colorectal anastomosis with omental flap creation.
Intraoperatively, the rectal mass was found to be fused to the posterior uterus. Histopathology confirmed rectovaginal endometriosis involving the rectal submucosa and muscularis propria, with no malignancy identified. The patient recovered well postoperatively, with resolution of GI symptoms.
Discussion:
This case highlights the importance of considering rectovaginal endometriosis in the differential diagnosis of rectal masses, particularly in women of reproductive age with inconclusive biopsies. Endoscopic and radiologic findings may closely mimic malignancy, and superficial biopsies often miss the diagnosis. A high index of suspicion, cross-sectional imaging, and collaboration with gynecology are essential. This case underscores that not all rectal masses are malignant; gynecologic etiologies such as endometriosis should be considered.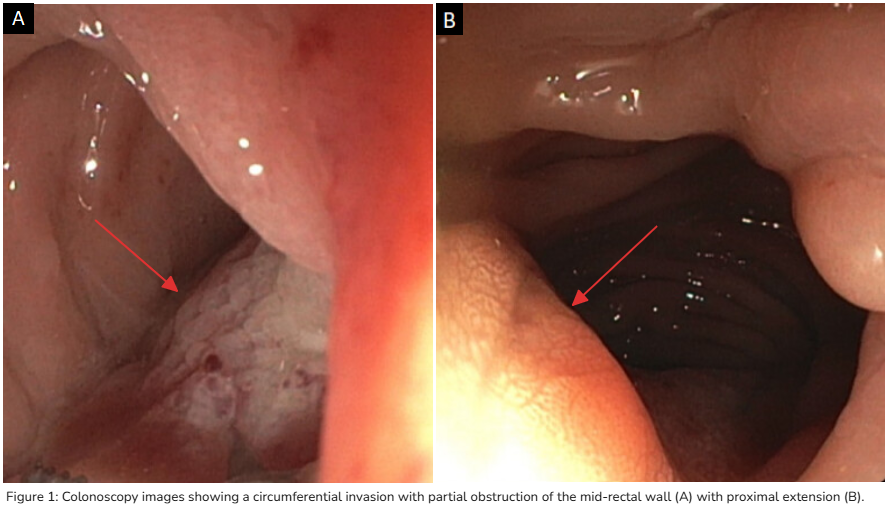
Figure: Figure 1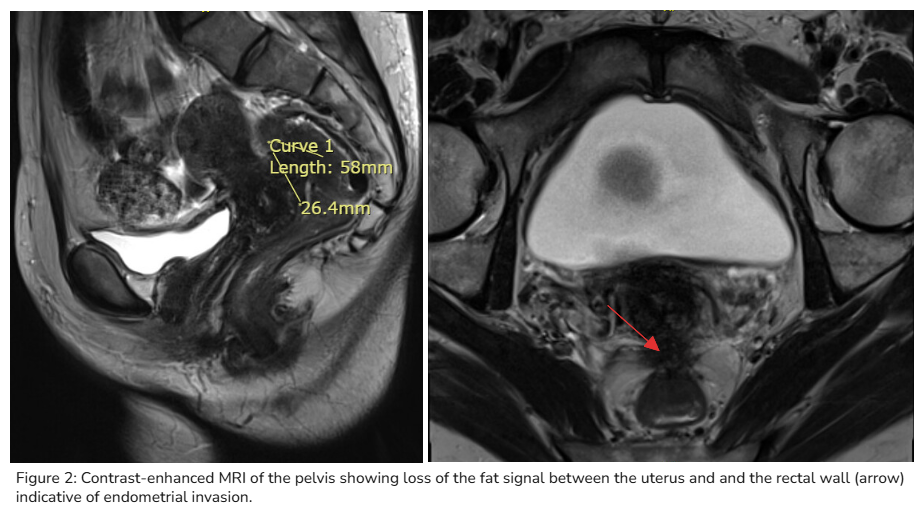
Figure: Figure 2
Disclosures:
Tasneem Jamal Al-Din indicated no relevant financial relationships.
Adrianna Wierzbicka indicated no relevant financial relationships.
Mariana Berho indicated no relevant financial relationships.
Giovanna da Silva indicated no relevant financial relationships.
Alison Schneider indicated no relevant financial relationships.
Andrew Ukleja indicated no relevant financial relationships.
Tasneem Jamal Al-Din, MD, Adrianna Wierzbicka, MD, Mariana Berho, MD, Giovanna da Silva, MD, Alison Schneider, MD, Andrew Ukleja, MD, CNSP. P4650 - Rectovaginal Endometriosis Masquerading as a Rectal Mass, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.