
Tuesday Poster Session
Category: Colon

Alex Chang, MD
Brown University / Rhode Island Hospital
Providence, RI
While squamous cell epithelium is thought to be present only in the anal canal in the lower GI tract, recent cases have described primary rectal squamous cell carcinoma (rSCC). Given the low incidence of rSCC, the pathogenesis, clinical presentation, and diagnosis is poorly understood. This case describes the presentation and diagnosis of rSCC.
Case Description/
Methods:
An 82-year old female presented to the emergency department with 2 months of hematochezia and maroon-colored stools along with 1 week of exertional dyspnea. She denied weight loss, fevers, or night sweats in the preceding months. A digital rectal exam demonstrated tenderness and a palpable mass.
Her medical history included atrial fibrillation on apixaban and prior lower GI bleeds thought to be from internal hemorrhoids. The inpatient GI team was consulted for a colonoscopy, which revealed a malignant stricture in the rectum, 10 cm from the anal verge. Biopsies demonstrated a moderately-differentiated, keratinizing, p16-mutated squamous cell carcinoma. Upon further interview, she noted no known history of HPV infection. She ultimately decided to forego any further workup or treatment.
Discussion: Differentiating primary rSCC from local spread of a primary cervical or anal canal tumor can be challenging. Morphologically, rSCC is indistinguishable from anal squamous cell carcinoma (SCC). Keratinization can occur in either malignancy; however, keratin 8 and 18 immunohistochemical stains can be helpful as they can be positive in rSCC but not in anal SCC. In this case, immunohistochemical staining was not completed. On colonoscopy, there was no evidence of continuation of the mass to the anal canal, more consistent with a primary rSCC.
Various theories exist for the pathogenesis of rSCC. The predominant theory involves initial metaplasia from chronic inflammation, or exposure to radiation or carcinogens. The possibility of ectopic patches of squamous epithelium has also been suggested. While HPV has been implicated in SCC of the cervical, anal, or oral tract, the role of HPV in the development of rectal SCC is unclear. While this patient had no known risk factors for squamous metaplasia and had previously not tested positive for HPV, the positive p16 mutation suggests HPV-induced malignant transformation rather than chronic rectal inflammation. More studies are needed to better understand rSCC pathogenesis.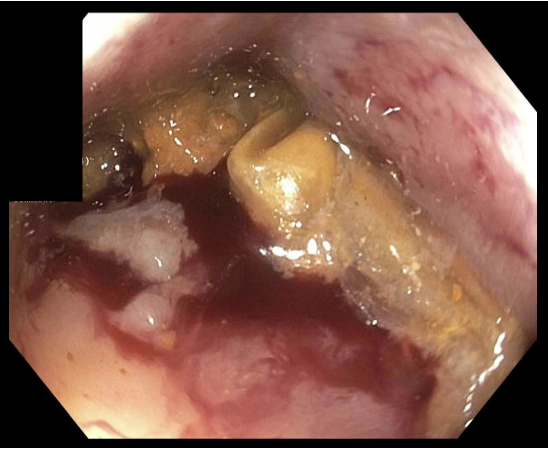
Figure: Figure 1 Colonoscopy Image of Rectal Stricture with Circumferential Narrowing and Ulceration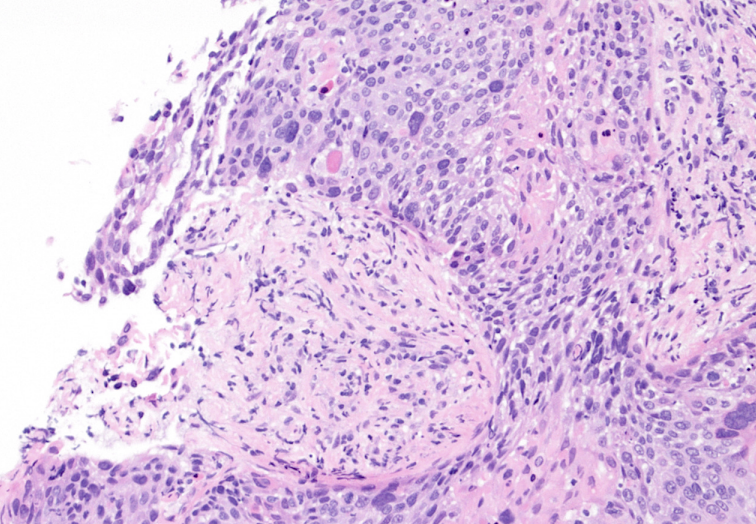
Figure: Figure 2 H&E Stain of Rectal Biopsy Showing Squamous Cell Carcinoma
Disclosures:
Alex Chang indicated no relevant financial relationships.
Kimberly Ho indicated no relevant financial relationships.
Andrew Petrou indicated no relevant financial relationships.
Daniel Kats indicated no relevant financial relationships.
Yousef Elfanagely indicated no relevant financial relationships.
Khaled Alkhateeb indicated no relevant financial relationships.
Li Wang indicated no relevant financial relationships.
Alex Chang, MD, Kimberly Ho, MD, Andrew Petrou, MD, Daniel Kats, MD, Yousef Elfanagely, MD, Khaled Alkhateeb, MBBS, Li Wang, MD. P4642 - p16 Mutated Primary Squamous Cell Carcinoma of the Rectum, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.