Walter Reed National Military Medical Center San Diego, CA
Award: ACG Presidential Poster Award
Jeffrey Kwan, MD1, John McCarthy, MD2, Robert Spiller, DO, MS2 1Walter Reed National Military Medical Center, San Diego, CA; 2Walter Reed National Military Medical Center, Bethesda, MD Introduction: Appendiceal intussusception or inversion (AI) is often an incidental endoscopic or radiographic finding. Presentations can range from asymptomatic to prolonged right lower quadrant abdominal pain. It is a rare finding with an estimated incidence of 1 in 10,000 patients who undergo appendectomy. An iatrogenic cause of AI is when the base of the appendix is inverted into the cecum during open appendectomy with a purse string suture.
Case Description/
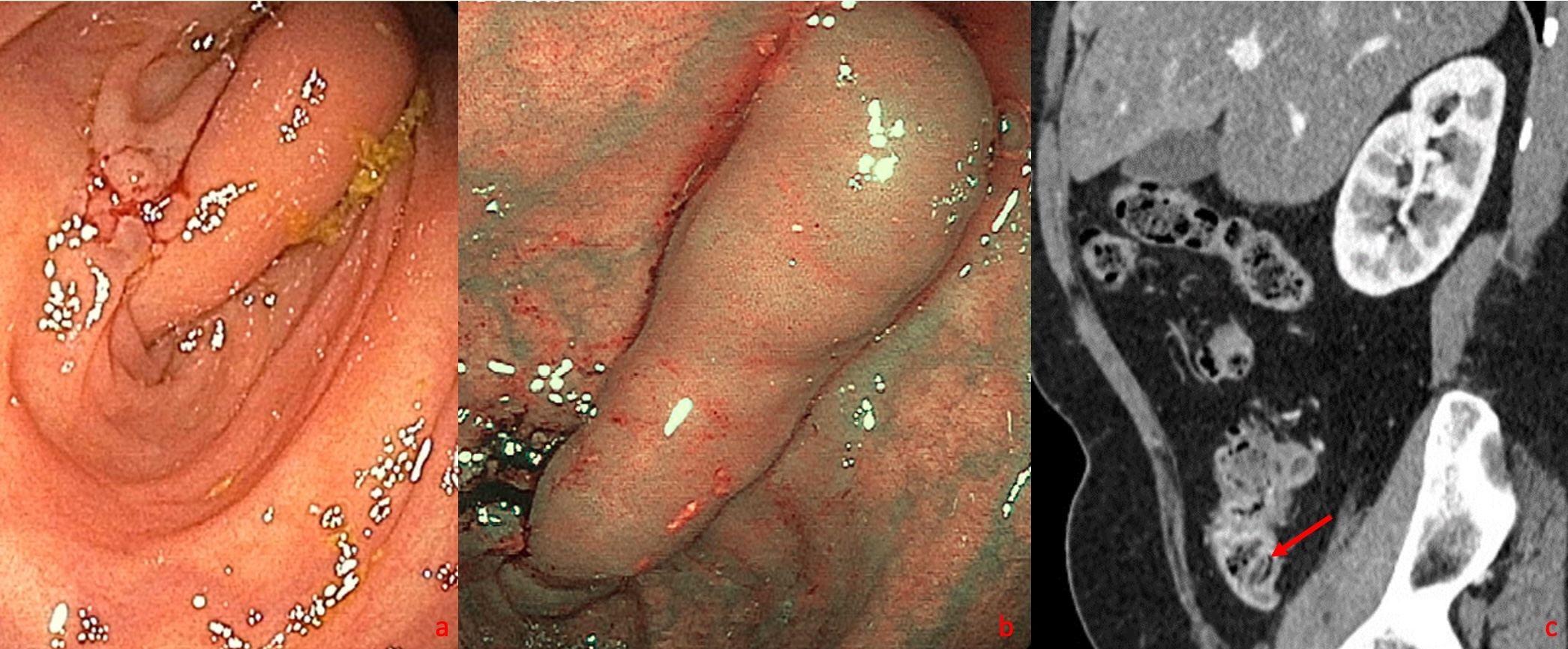
Methods: A 62-year-old female with congenital epispadias requiring extensive surgeries presented to primary care with non-specific episodic right flank pain. On non-contrast CT, she was found to have punctate non-obstructing nephroliths and no visualized appendix. She had no prior colon cancer screening and subsequently underwent colonoscopy which showed a large, mobile, cecal mass. (Fig. 1a/b) Upon further inspection, it appeared to emanate from the appendiceal orifice and deemed to be an inverted appendix. In reviewing her endoscopic findings, the patient reported she had an appendectomy during total abdominal hysterectomy in 1985. A CT with oral and IV contrast was performed which confirmed the finding of an inverted appendix. (Fig. 1c) Given these findings and ongoing symptoms, considerations for surgical versus endoscopic appendectomy were considered.Prior to proceeding, the surgical report from 1985 was able to be reviewed which stated that the appendix was transected and the remaining appendiceal stump had been inverted into the cecum.Additional prior CT results from this timeframe were also reviewed and confirmed this finding to be present for decades and thus less likely to be the source of her subacute episodic abdominal pain. Discussion: After discovery of a cecal mass at the appendiceal orifice during colonoscopy, it is important to consider an inverted appendix.CT scan with contrast can aid in ruling out other sinister mimickers at the appendiceal orifice such as appendiceal mucinous adenocarcinoma. Mucosal biopsies are rarely helpful given normal overlying mucosa.Failing to distinguish an AI from a subepithelial lesion (SEL) or mucosal polyp can lead to unnecessary removal and potential complication if removed using standard polypectomy techniques.Most AI are asymptomatic, and thus judicious review of prior abdominal surgeries and CT scans should occur prior to attributing symptoms to this finding. Surgical management versus endoscopic removal should be reserved for patients who demonstrate symptoms related to AI.
Figure: Figure 1a. Inverted appendix visualized at the appendiceal orifice. Figure 1b. NBI of inverted appendix showing normal appearing mucosa without hypervascularity. Figure 1c. Sagittal view of CT Abdomen/Pelvis w/ contrast showing inverted appendix in the cecum.
Disclosures: Jeffrey Kwan indicated no relevant financial relationships. John McCarthy indicated no relevant financial relationships. Robert Spiller indicated no relevant financial relationships.
Jeffrey Kwan, MD1, John McCarthy, MD2, Robert Spiller, DO, MS2. P4637 - Not a Polyp! Do Not Get Twisted by Appendiceal Inversion, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.