University of Maryland Medical Center Baltimore, MD
Rosemary Ansah, MBChB, MPH, Ebehiwele Ebhohon, MBBS, MPH, MsCr, William Twaddell, MD, Zurabi Lominadze, MD University of Maryland Medical Center, Baltimore, MD Introduction: Autoimmune hepatitis (AIH) is a chronic inflammatory liver disease that typically affects middle-aged women. Atypical presentations in young males and overlap with viral or genetic factors can obscure diagnosis. We present a case of AIH in a young man with presumed EBV hepatitis and a heterozygous C282Y mutation for hemochromatosis.
Case Description/
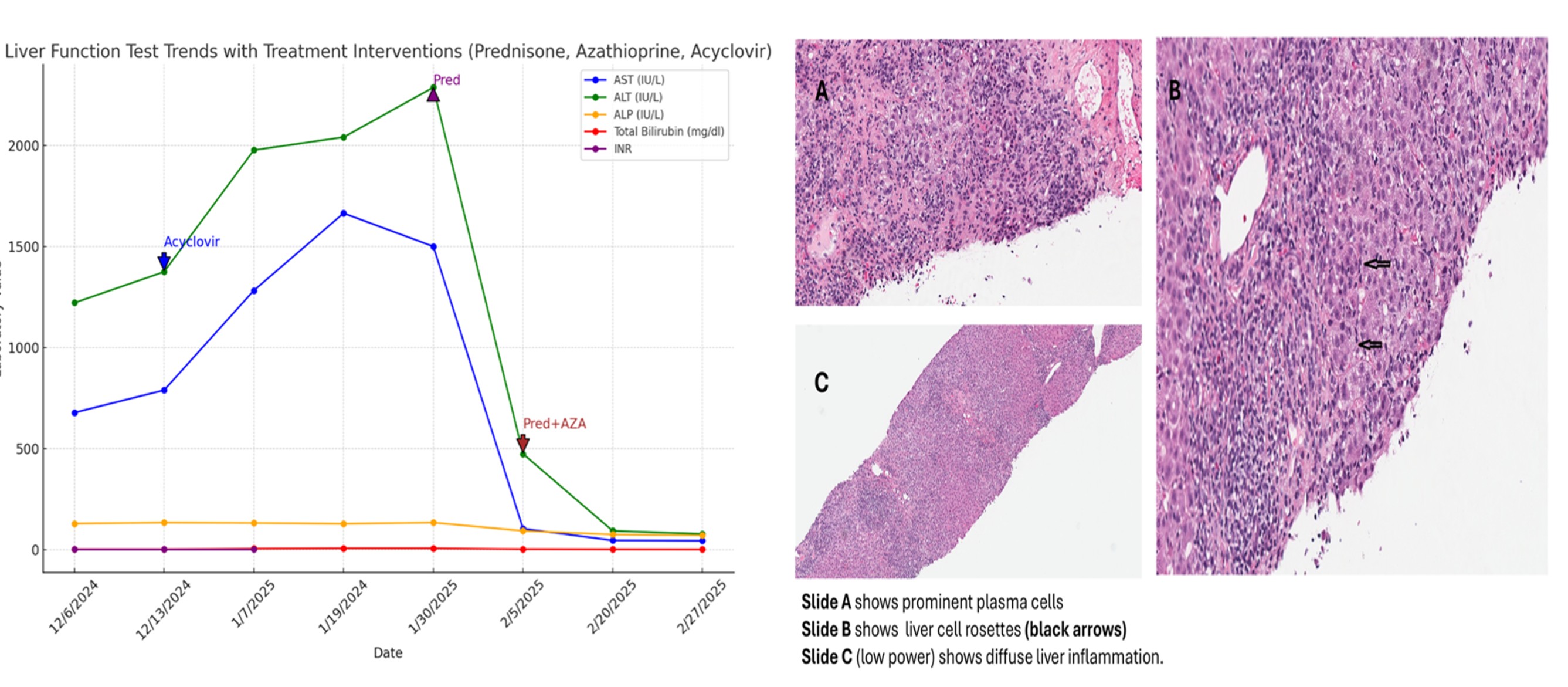
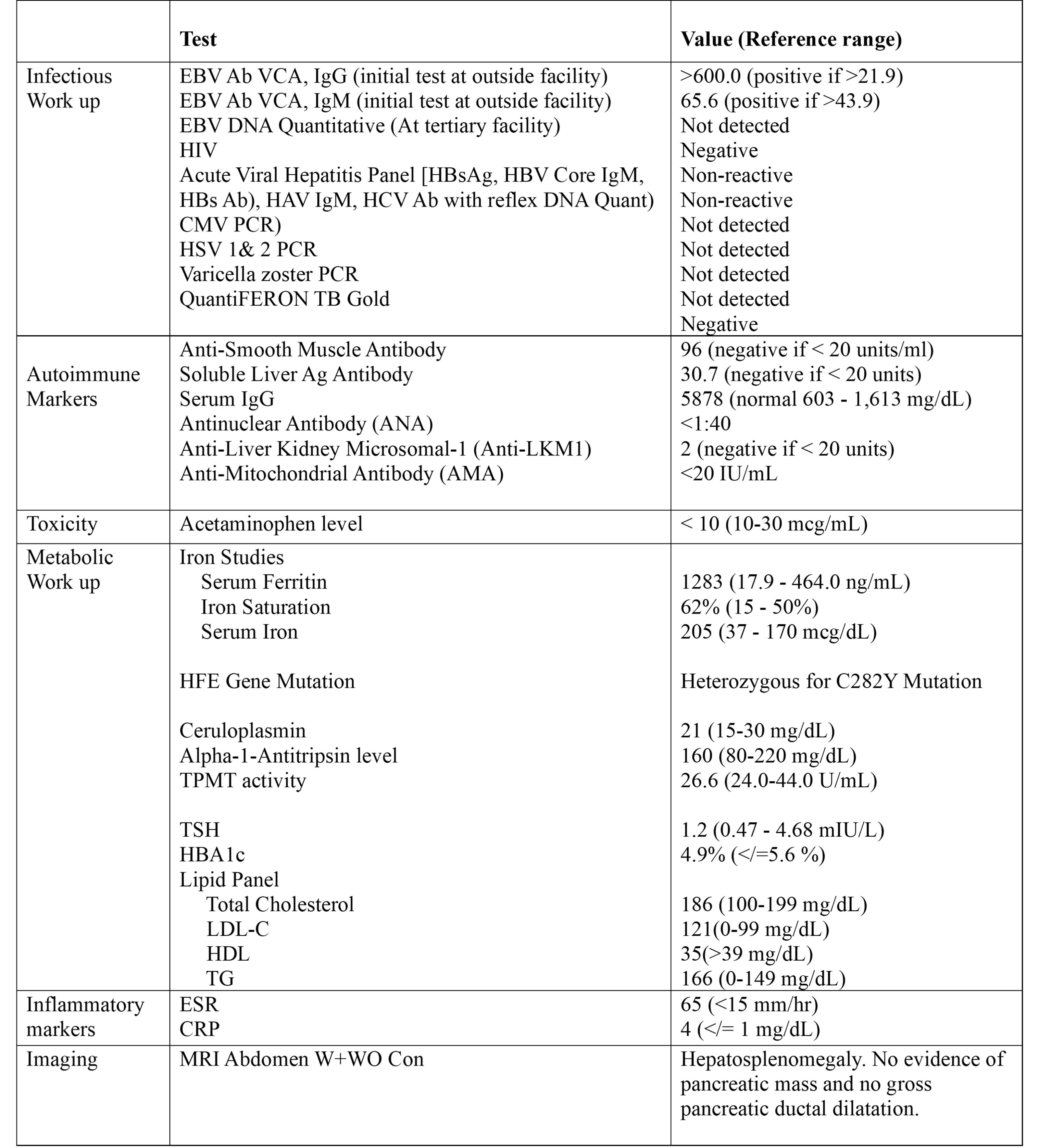
Methods: A 30-year-old male with no prior liver disease presented for routine wellness care and was incidentally found to have elevated AST (678) and ALT (1221). He denied use of alcohol, smoking, IV drugs, tattoos, OTC medications or herbal supplements. He denied recent international travel. Family history was positive for hemochromatosis in his father. Initial labs noted positive EBV IgG and IgM, and transaminase elevations were attributed to presumed EBV hepatitis. Despite a 10-day course of acyclovir, liver enzymes worsened, peaking at ALT 2286 and AST >1500. Due to jaundice, he went to an ER where imaging showed hepatosplenomegaly, gallbladder distention, and porta hepatis lymphadenopathy, and thereafter was referred to our tertiary center due to concern for acute liver injury. Subsequent evaluation revealed serum ferritin 1283 ng/ml, serum iron 205, heterozygous C282Y mutation, positive ASMA, Anti-SLA/AP levels, and elevated serum IgG levels. EBV DNA Quantitative was negative when checked at this time. A liver biopsy revealed interface hepatitis with plasma cells, rosettes, and hemosiderin-laden Kupffer cells, consistent with AIH (activity 3/4, fibrosis 2/4). IgG was markedly elevated to 5878. He was treated with IV methylprednisolone followed by oral prednisone and azathioprine, with rapid clinical and biochemical improvement. Discussion: This case highlights the diagnostic complexity of AIH in the context of EBV hepatitis and a carrier state for hemochromatosis. EBV can transiently elevate liver enzymes and obscure autoimmune etiologies. Hemosiderin on liver biopsy in a C282Y heterozygote further complicates interpretation. The patient's positive response to standard immunosuppression supports the diagnosis of AIH despite the confounding factors of viral infection and iron deposition.