University of Tennessee Health Science Center Chattanooga, TN
Haseeb Mohideen, MD, James Laney, MD, James Pitcher, MD, Laxmi Parsa, MD University of Tennessee Health Science Center, Chattanooga, TN Introduction: Small bowel obstruction in adults can have various etiologies including peptic strictures, malignancy, and Crohn’s disease; however, obstruction in children typically occurs due to congenital abnormalities such as atresia or stenosis. In rare instances, a septum within the small bowel, either acquired or congenital, can lead to intermittent obstruction that manifests in adulthood.
Case Description/
Methods: A 53-year-old female presented to the emergency department due to sudden-onset abdominal pain, nausea, and vomiting for three days. Her vitals were stable, and physical exam was only notable for epigastric distension. CT demonstrated a distended, fluid-filled stomach and duodenal bulb despite the patient reporting no oral intake for over 12 hours. On review, the patient had recurrent presentations for similar symptoms that would resolve with supportive measures, and imaging during those presentations was also notable for similar distension. She reported that between episodes she was asymptomatic. An outpatient gastric emptying study demonstrated normal gastric emptying. EGD revealed a thick septum dividing the lumen of the second portion of the duodenum. Each orifice could be traversed, but resistance to adult gastroscope passage was observed. The patient was presumed to have recurrent duodenal obstruction secondary to the septum. Endoscopic intervention or surgical evaluation was offered, but she elected to pursue conservative management. A low-residue diet was initiated, and at follow-up, she denied any recurrence of symptoms. Discussion: Septa within the GI tract can be congenital or acquired. Congenital septa are typically diagnosed in infancy due to small bowel obstruction. In rare instances, a partially occlusive septum can lead to delayed presentation in adulthood. Acquired septa of the GI tract can occur due to penetrating ulceration with fistula formation resulting in the appearance of two lumens. Imaging is typically nonspecific, revealing features of gastric outlet or bowel obstruction; however, endoscopy would reveal a septum with stenosis. Once a septum is identified as an etiology of stenosis or obstruction, most patients will require endoscopic or surgical intervention. However, conservative management with dietary modification can be attempted in patients with mild symptoms. Endoscopic management may consist of balloon dilation, stent placement, or hook knife incision. In cases of severe stenosis or obstruction, surgical resection or duodenoplasty may be necessary.
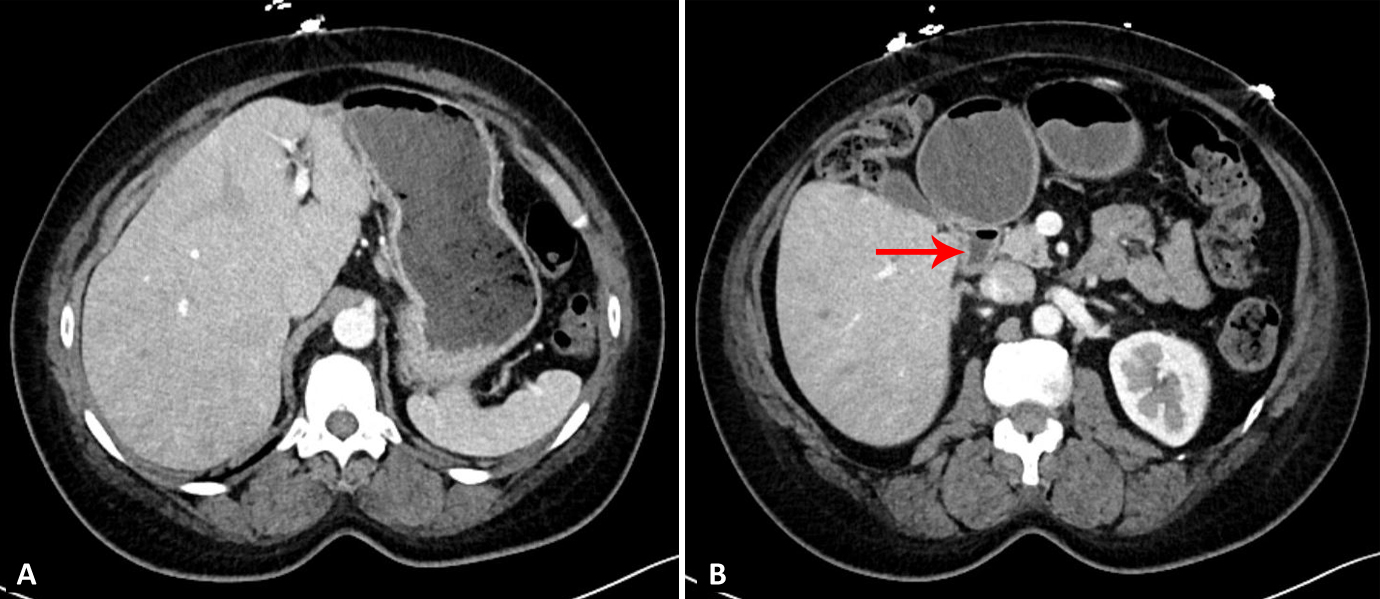
Figure: Figure 1: Abdominal CT demonstrating a distended, fluid-filled stomach (A) and duodenal bulb (B, red arrow).
Figure: Figure 2: EGD demonstrating a septum dividing the lumen of the second portion of the duodenum.
Disclosures: Haseeb Mohideen indicated no relevant financial relationships. James Laney indicated no relevant financial relationships. James Pitcher indicated no relevant financial relationships. Laxmi Parsa indicated no relevant financial relationships.
Haseeb Mohideen, MD, James Laney, MD, James Pitcher, MD, Laxmi Parsa, MD. P6230 - Double-Lumen Duodenum: A Septum Leading to Small Bowel Obstruction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")