Prajjwol D. Bhatta, MD1, John Shrestha, MBBS2, Mahesh Nepal, MD1, Asim Mushtaq, MD3, Hamza Akhtar, MD1 1Rochester General Hospital, Rochester, NY; 2Rochester General hospital, Rochester, NY; 3Rochester Regional Health, Rochester, NY Introduction: Eosinophilic gastrointestinal diseases (EGIDs) are broadly classified into eosinophilic esophagitis (EoE) and non-eosinophilic esophagitis eosinophilic gastrointestinal disease (non-EoE-EGID) based on the gastrointestinal segments involved. Non-EoE-EGIDS estimated prevalence is fewer than 10 cases per 100000 individuals whereas prevalence of Eosinophilic gastritis/Eosinophilic enteritis is 5.1/100,000 people. 41% show eosinophilic inflammation beyond the primary site, often the esophagus. We present a rare case of EoE with EoG/EoN presenting as pyloric stenosis.
Case Description/
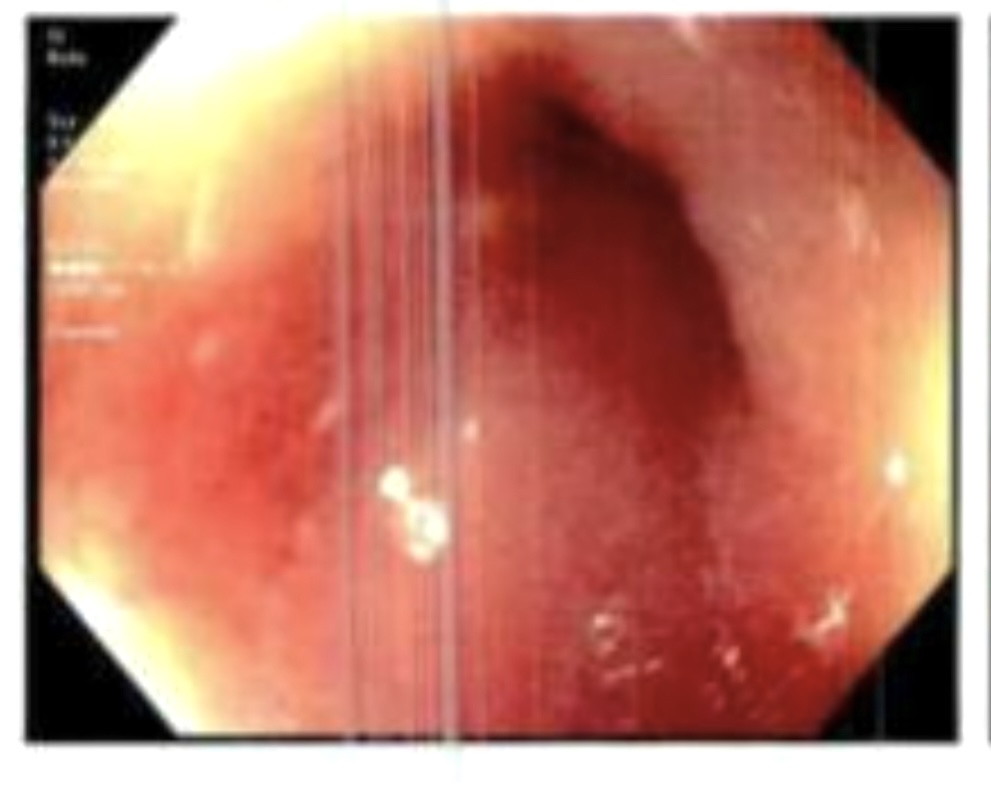
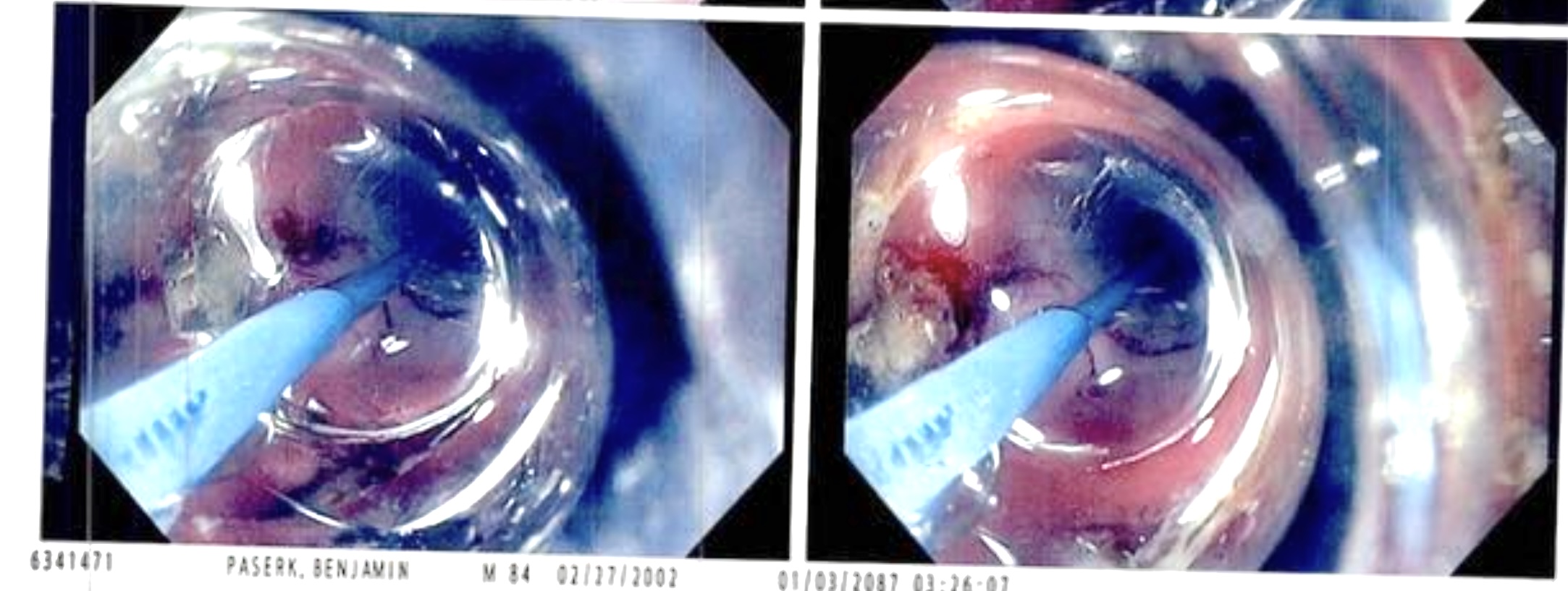
Methods: A 22-year-old male presented with 8 months of abdominal pain, frequent vomiting, and 70 lbs weight loss. Initial EGD demonstrated LA grade D esophagitis with linear furrows suspicious for eosinophilic esophagitis in mid and distal esophagus and large amount of bezoar in the stomach. Histopathology revealed patchy increased intraepithelial eosinophils, with peak count >80/HPF, along with eosinophilic micro abscesses. A repeat EGD 8 weeks later showed LA grade B with persistent linear furrows in mid and distal esophagus with severe pyloric stenosis with abnormal surrounding mucosa. Biopsy of the pyloric region revealed increased eosinophils up to 200/HPF in lamina propria. Allergy and immunology were consulted, and the patient was initiated on Dupilumab 300 mg weekly for eosinophilic gastritis leading to improvement in nausea and vomiting. Patient underwent multiple sessions of fluoroscopy-guided balloon dilation for pyloric stenosis. Discussion: This case illustrated the diagnostic and therapeutic complexity of EGIDs. In our patient, eosinophil infiltration was noted in lamina propria but not in muscularis layer, which contrasts with prior studies. The eosinophil count at the pyloric stenosis site in our patient reached up to 200/HPF, significantly exceeding threshold proposed in prior literature. There is a lack of consensus-accepted thresholds for the diagnosis of non-EoE-EGIDS. Unfortunately, no specific sensitive blood biomarkers have been reported for diagnosing adult cases with non-EoE-EGID or severity assessment. Standard treatment options exist for EoE, but there are no established treatment guidelines and no approved treatments for EoG and EoN. This case highlights the diagnostic challenges and variable histopathological patterns in non-EoE-EGID, emphasizing the need for standardized diagnostic criteria and tailored therapeutic approaches.
Figure: Figure1: Pyloric stenosis
Figure: Figure2: Fluoroscopically guided CRE balloon dilation of pyloric stenosis
Disclosures: Prajjwol Bhatta indicated no relevant financial relationships. John Shrestha indicated no relevant financial relationships. Mahesh Nepal indicated no relevant financial relationships. Asim Mushtaq indicated no relevant financial relationships. Hamza Akhtar indicated no relevant financial relationships.
Prajjwol D. Bhatta, MD1, John Shrestha, MBBS2, Mahesh Nepal, MD1, Asim Mushtaq, MD3, Hamza Akhtar, MD1. P6303 - Concurrent Eosinophilic Esophagitis and Eosinophilic Gastroenteritis Presenting with Gastric Outlet Obstruction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.