Montefiore St Luke's Cornwall Hospital Newburgh, NY
Anastasiia Babintseva, MD1, Suchith Boodegere Suresh, 1, Veronica Manchanda, MD1, Polina Korsukova, MD2 1Montefiore St Luke's Cornwall Hospital, Newburgh, NY; 2Pirogov Russian National Research Medical University, Boston, MA Introduction: Kaposi sarcoma (KS) is a rare AIDS-defining malignancy caused by human herpesvirus 8 (HHV-8). While it classically presents with cutaneous lesions, visceral involvement—particularly in the gastrointestinal tract—can occur without skin findings. Recognition is critical, especially in severely immunocompromised patients presenting with unexplained symptoms such as chest pain or anemia.
Case Description/
Methods: A 46-year-old incarcerated male with HIV (noncompliant with ART), asthma, seizure disorder, substance use, and a recent pulmonary embolism on apixaban presented with a chief complaint of persistent left-sided chest pain and shortness of breath, worsened when lying on his right side. He also reported blood-tinged vomiting and one episode of black semi-formed stool. He had been discharged two weeks earlier from an outside facility on apixaban after a diagnosis of a small pulmonary embolism. Vitals revealed tachycardia (HR 103), with stable blood pressure and oxygenation. Labs showed normochromic anemia (Hb 8.3 g/dL, down from 11 g/dL two months prior), iron 18 µg/dL, iron saturation 7%, INR 1.69. CT chest ruled out recurrent PE and showed a trace pericardial effusion. Troponin and EKG were unremarkable. Gastroenterology was consulted. Esophagogastroduodenoscopy revealed multiple violaceous nodules in the gastric antrum and white plaques in the esophagus. Colonoscopy was attempted but was unsuccessful due to inadequate bowel preparation, which limited mucosal visualization. Gastric biopsy showed benign ulcerated mucosa with chronic active gastritis and was diffusely positive for HHV-8, consistent with Kaposi sarcoma. Esophageal biopsy confirmed pronounced candidal esophagitis with numerous pseudohyphae. CD4 count was 23 (2%) with a CD4:CD8 ratio of 0.03. He was treated with IV iron and oral fluconazole and discharged on ferrous sulfate, apixaban, and ART. He remained stable without transfusion. Referral to Hematology/Oncology arranged. Discussion: Gastrointestinal Kaposi sarcoma is rare and usually seen with cutaneous lesions. Our patient had no external signs, making the diagnosis challenging. Visceral involvement may present with nonspecific symptoms like anemia, bleeding, or abdominal discomfort and may mimic gastritis or ulcers. In this case, endoscopy with biopsy and HHV-8 staining was essential. Coexisting candidal esophagitis reflected profound immunosuppression. Early endoscopy in high-risk HIV patients is key to identifying occult GI Kaposi sarcoma and guiding timely treatment.
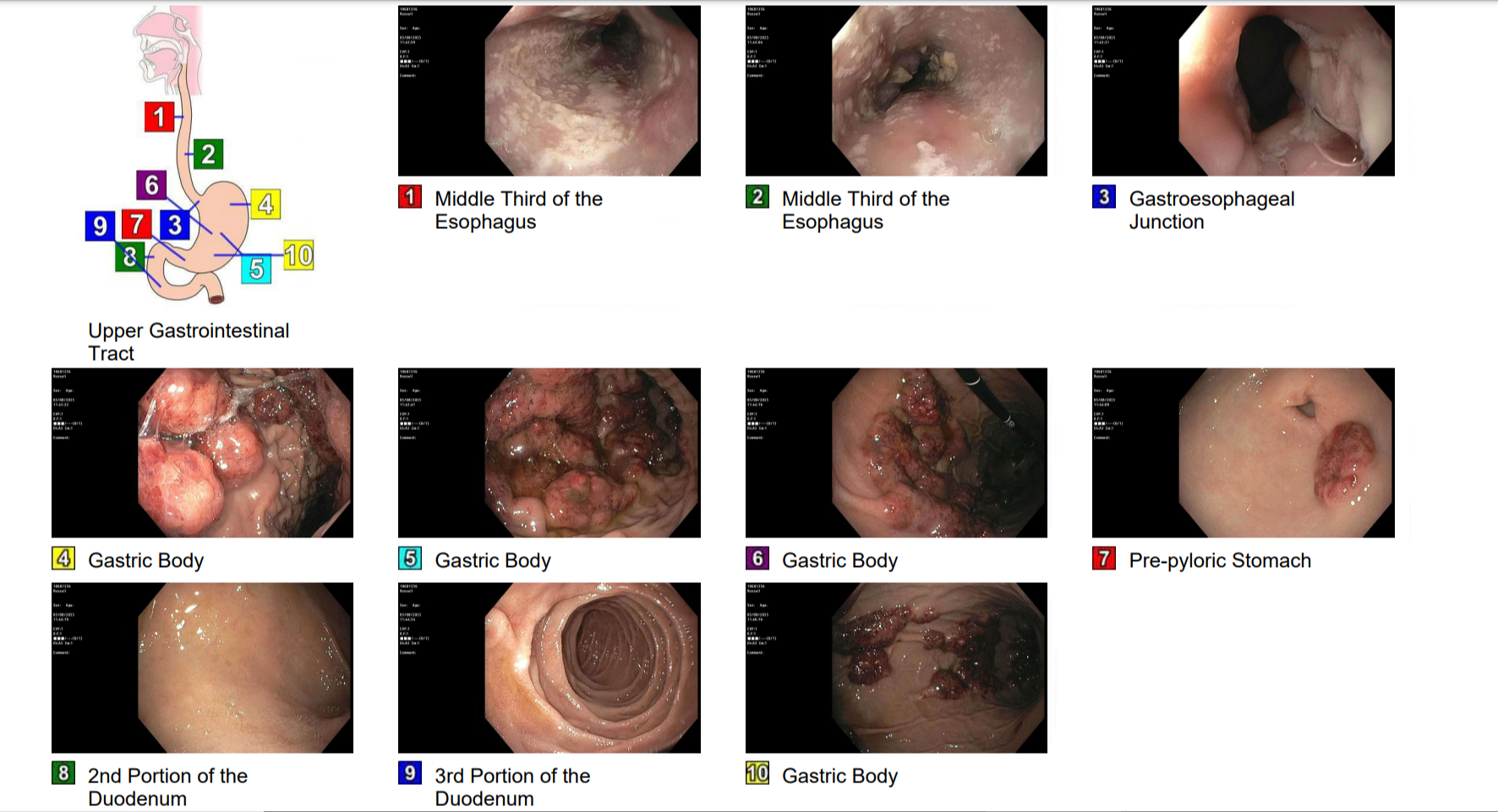
Figure: Endoscopic images demonstrating multiple violaceous nodular lesions in the gastric body (Panels 4–6, 10), consistent with Kaposi sarcoma, and white plaques in the mid-esophagus (Panels 1–2), consistent with candidal esophagitis.
Disclosures: Anastasiia Babintseva indicated no relevant financial relationships. Suchith Boodegere Suresh indicated no relevant financial relationships. Veronica Manchanda indicated no relevant financial relationships. Polina Korsukova indicated no relevant financial relationships.
Anastasiia Babintseva, MD1, Suchith Boodegere Suresh, 1, Veronica Manchanda, MD1, Polina Korsukova, MD2. P6381 - Gastric Kaposi Sarcoma Presenting as Chest Pain, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.