SSM Health Saint Louis University Hospital St. Louis, MO
Isra N. Taha, MD1, Nitin Desai, MD2, Spyridon Zouridis, MD1, Danielle Carpenter, MD1, Kelly Fan, MD1, Mike Giacaman, MD2 1SSM Health Saint Louis University Hospital, St. Louis, MO; 2Saint Louis University, Saint Louis, MO Introduction: Kaposi sarcoma (KS), a vascular tumor caused by human herpesvirus 8 (HHV8) and an autoimmune immunodeficiency syndrome (AIDS)-defining illness, is one of the most common gastric malignancies in patients with human immunodeficiency virus (HIV). Gastric KS without cutaneous lesions is extremely rare. We describe a patient with HIV and chronic gastrointestinal (GI) symptoms who was ultimately diagnosed with gastric KS despite lack of mucocutaneous involvement. This case highlights the presentation and evaluation, particularly in the context of complex comorbidities that may make diagnosis challenging.
Case Description/
Methods: A 52-year-old African American male with advanced HIV (CD4 count of 92),no prior AIDS-defining illnesses, poor antiretroviral (ART) adherence, chronic hepatitis B, cytomegalovirus (CMV) viremia, alcohol use disorder, heart failure, and anal cancer presented with a 12-month history of fatigue, malnutrition, weight loss, and diarrhea. Esophagogastroduodenoscopy (EGD) and colonoscopy showed mild gastric mucosal inflammation and colonic tubular adenomas. He presented 6 months later with loss of appetite and emesis. Imaging showed steatosis, mesenteric lymphadenopathy, colitis, and cholecystitis; extensive infectious workup was negative. Repeat EGD showed multiple raised, hypervascular nodules with central erosion in the gastric fundus and body; biopsies showed inflammation, reactive changes, and spindled vascular lesions staining positive for CD31 and HHV8, confirming gastric KS. He was discharged on highly active antiretroviral therapy (HAART) with plans to follow-up with infectious diseases and oncology. Systemic chemotherapy was not indicated based on limited KS disease burden; this was to be re-evaluated once HIV was further controlled. Discussion: It is essential to maintain a high suspicion for KS in HIV patients with GI symptoms, even in the absence of cutaneous lesions. The standard of diagnosis is endoscopy, which may show classic maculopapular violaceous lesions or polypoid/nodular lesions, and biopsy with confirmatory immunohistochemical staining. Treatment options include ART, systemic chemotherapy, and symptom palliation. Prognosis depends on the severity and extent of disease. This case of isolated gastric KS in a patient with poorly controlled HIV and multiple other comorbidities demonstrates the significance of histopathology in confirming the diagnosis and emphasizes the role of multi-disciplinary collaboration in managing these complex clinical scenarios.
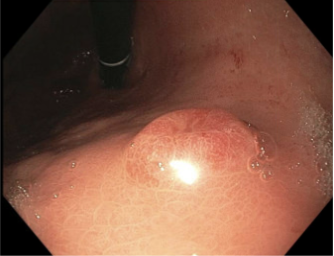
Figure: Endoscopic appearance of gastric body nodule with erosion and hypervascularity
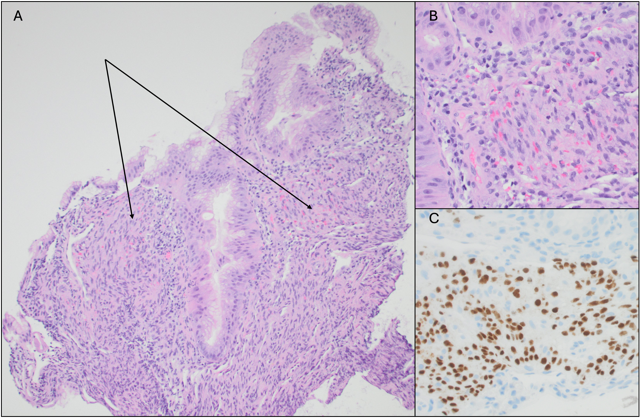
Figure: A: Gastric mucosa with spindled proliferation in the lamina propria (arrows) B: Extravasated RBCs evident at higher magnification C: Positive nuclear staining by HHV8 immunostain
Disclosures: Isra Taha indicated no relevant financial relationships. Nitin Desai indicated no relevant financial relationships. Spyridon Zouridis indicated no relevant financial relationships. Danielle Carpenter indicated no relevant financial relationships. Kelly Fan indicated no relevant financial relationships. Mike Giacaman indicated no relevant financial relationships.
Isra N. Taha, MD1, Nitin Desai, MD2, Spyridon Zouridis, MD1, Danielle Carpenter, MD1, Kelly Fan, MD1, Mike Giacaman, MD2. P6368 - A Rare Case of Primary Gastric Kaposi Sarcoma Without Mucocutaneous Involvement in a Patient With Advanced HIV, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.