NYC Health + Hospitals/South Brooklyn Health Brooklyn, NY
Award: ACG Presidential Poster Award
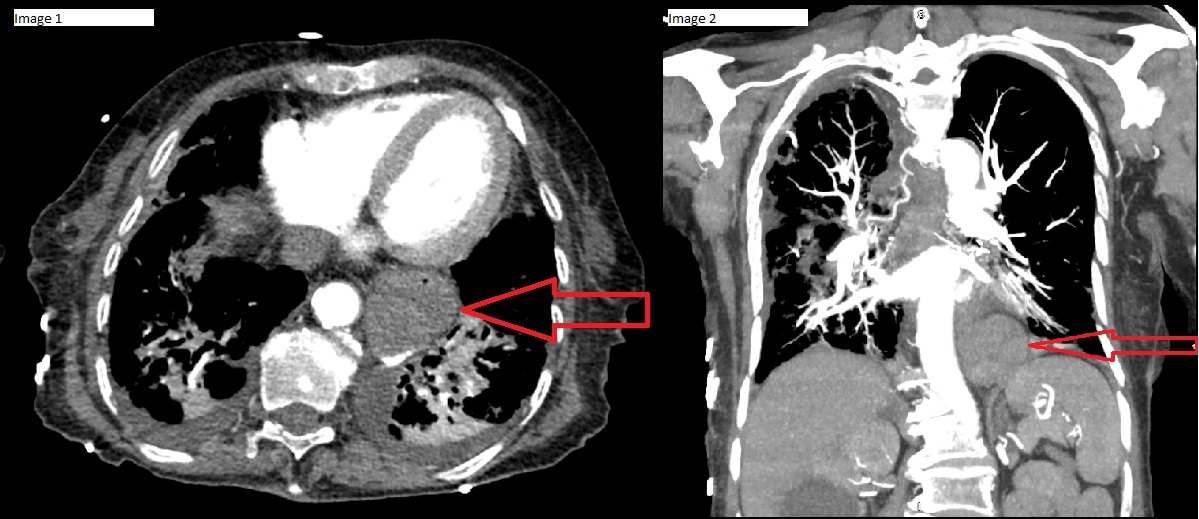
Bishoy Boulus Elkoumes, MD1, Joel Gabin Konlack Mekontso, MD2, Sara Samad, DO1, Justin Wagner, DO1, John Trillo, MD1 1NYC Health + Hospitals/South Brooklyn Health, Brooklyn, NY; 2New York City Health and Hospitals, South Brooklyn Health, New York, NY Introduction: Hiatal hernia (HH) is the protrusion of part of the stomach through the esophageal hiatus. 60% of the population > 50 years of age have HH, more evident in women, however, only 10% present with symptoms (esophageal and extraesophageal). Cardiac arrhythmia is a serious and rare complication that can be caused by HH due to direct compression on the heart, affecting the electrophysiology, or increased intrathoracic pressure.
Case Description/
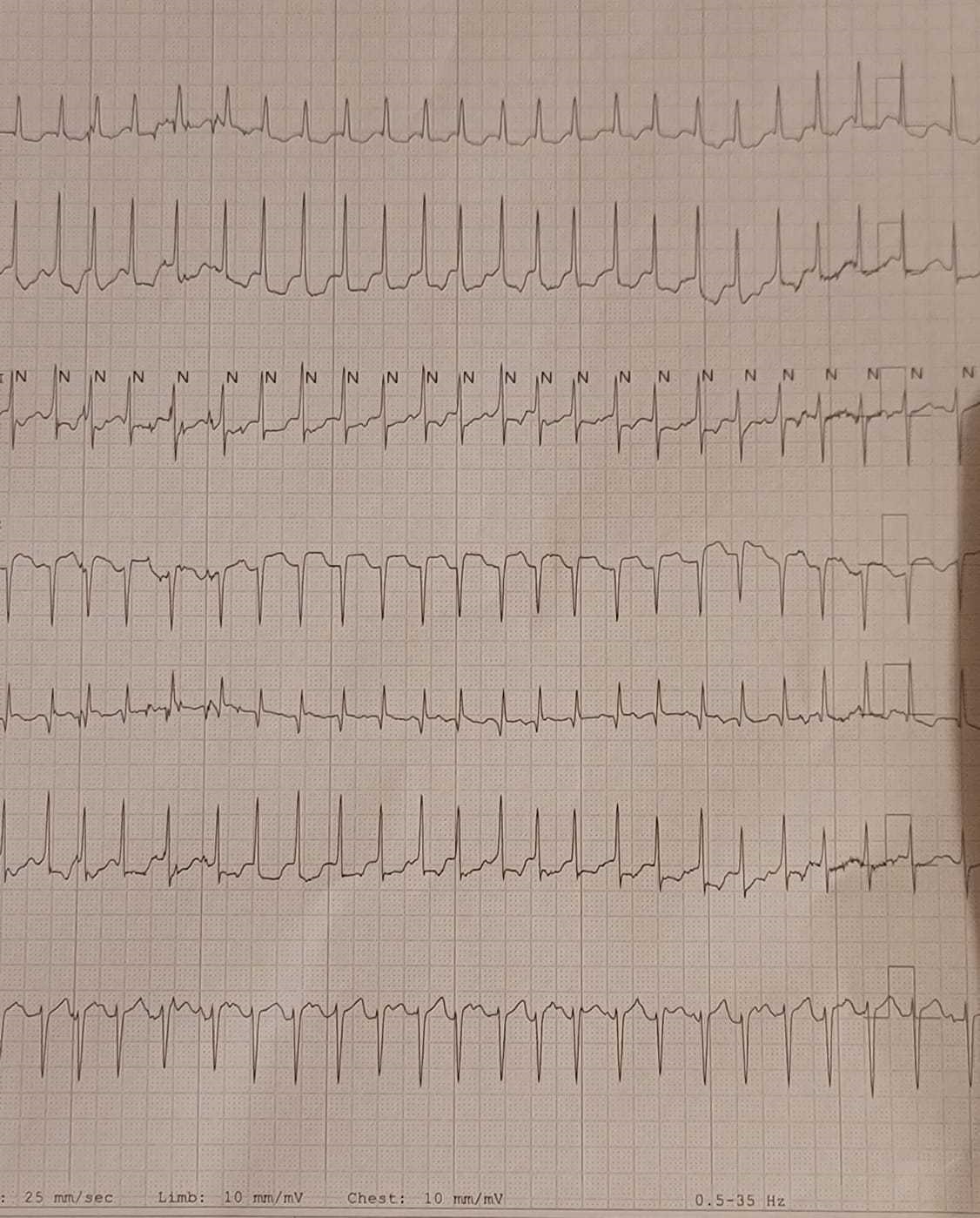
Methods: We present an 80-year-old female, with a past medical history of hypertension, chronic obstructive pulmonary disease and hiatal hernia who was brought in by her family for acute onset of shortness of breath and ultimately admitted to the intensive care unit for the management of acute hypoxic and hypercapnic respiratory failure and septic shock secondary to pneumonia, requiring intubation. The decision to place a central venous catheter (CVC) was made for infusion of high volume of fluids and pressors support. Prior to the procedure, she was placed in Trendelenburg position, and the bedside monitor showed tachycardia >220 beats per minute (BPM), unresponsive to carotid sinus massage or intravenous metoprolol injection. The telemetry strips were consistent with AVNRT. The patient was placed back in supine position, with head on bed elevation, which caused resolution of the arrhythmia. Discussion: Arrhythmias are a common condition that affects sick elderly hospitalized patients, usually, caused by dehydration, electrolytes disturbances or sepsis. However, in the aforementioned patient, none of these factors played a key role. Patient’s arrhythmia was triggered only when she was placed in Trendelenburg position for the CVC placement, and promptly resolved only with repositioning to the semi-sitting position. AVNRT reoccurred once the patient was placed again in Trendelenburg position, which infers that this was the only trigger for the arrhythmia. HH is a common benign finding on imaging, usually asymptomatic. Symptoms vary between esophageal (heartburn, regurgitation and dysphagia) and extraesophageal symptoms (chronic cough or asthma). However, moderate to large sized HH can manifest as life threatening arrhythmia. On literature review, 2 patients had resolution of premature ventricular complexes after, and atrial fibrillation resolution in an 80-year-old female, after surgical repair of HH. Multiple hypotheses claim that arrhythmia can be caused by extending inflammation to the left atrium, or ischemia caused by persistent atrial compression.
Disclosures: Bishoy Boulus Elkoumes indicated no relevant financial relationships. Joel Gabin Konlack Mekontso indicated no relevant financial relationships. Sara Samad indicated no relevant financial relationships. Justin Wagner indicated no relevant financial relationships. John Trillo indicated no relevant financial relationships.
Bishoy Boulus Elkoumes, MD1, Joel Gabin Konlack Mekontso, MD2, Sara Samad, DO1, Justin Wagner, DO1, John Trillo, MD1. P6409 - Hiatal Hernia-Induced Atrioventricular Nodal Reentry Tachycardia: A Case Report of a Rare Positional Arrhythmia in an Elderly Patient, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")