Julio D. Vega-Torres, MD, PhD1, Adrian R. Chico-Moya, MD2, Jose Martin-Ortiz, MD, FACG2 1VA Caribbean Healthcare System, Sabana Grande, Puerto Rico; 2VA Caribbean Healthcare System, San Juan, Puerto Rico Introduction: Linitis plastica is a rare and aggressive form of diffuse-type gastric adenocarcinoma, characterized by submucosal infiltration with minimal mucosal changes, which often leads to delayed diagnosis and advanced presentations, such as peritoneal carcinomatosis. Early detection remains challenging, as conventional imaging and endoscopy may be inconclusive. Immunohistochemical staining and molecular profiling are increasingly vital in determining tumor origin and guiding management. Here, we report a case of linitis plastica initially presenting as peritoneal carcinomatosis in a patient with a complex oncologic history.
Case Description/
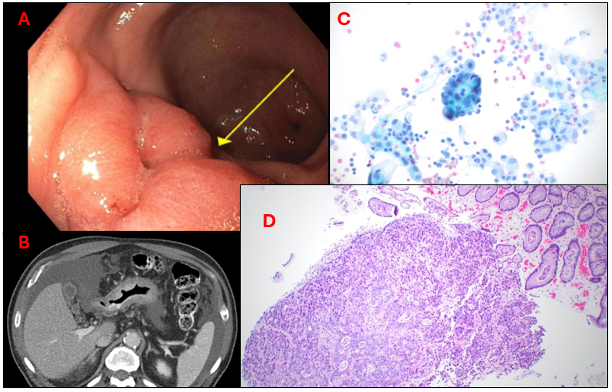
Methods: A 77-year-old male with prior prostate adenocarcinoma and recurrent colonic tubular adenomas presented with anorexia, weight loss, and abdominal discomfort. Serial colonoscopies (2018–2023) identified multiple adenomas and inflammatory polyps. CT imaging in late 2023 revealed a bulging appendix, raising concern for mucocele. Diagnostic laparoscopy in early 2024 showed diffuse peritoneal carcinomatosis and malignant ascites (Fig. 1C). Peritoneal biopsies revealed poorly differentiated adenocarcinoma positive for CK7 and CDX2 and negative for CK20, SATB2, and NKX3.1, favoring an upper gastrointestinal origin over colorectal or prostatic. Next-generation sequencing identified a MAP2K1 (MEK1) F53L mutation associated with diffuse-type gastric cancer. The patient began treatment with FOLFOX. A non-diagnostic initial endoscopic gastroduodenoscopy (EGD) was followed by a repeat endoscopy in May 2025, which revealed an antral mass (Fig. 1A). Biopsy confirmed poorly differentiated gastric adenocarcinoma, consistent with linitis plastica (Fig. 1D). Given disease progression, second-line therapy with ramucirumab and paclitaxel was initiated. Discussion: This case highlights the diagnostic challenges of linitis plastica, especially in patients with overlapping malignancies and inconclusive initial workups. Immunohistochemistry and molecular profiling—particularly MAP2K1 mutations—can provide diagnostic clarity and therapeutic direction. Imaging, repeat endoscopy, and biopsy remain essential in suspected gastric malignancy when initial studies are negative (Fig. 1A-D). Early consideration of linitis plastica in cases of peritoneal carcinomatosis may expedite diagnosis and improve management strategies.
Figure: Figure 1. Multimodal diagnostic findings in a patient with metastatic gastric adenocarcinoma. (A) Esophagogastroduodenoscopy (EGD) showing subtle mucosal irregularity in the gastric antrum (yellow arrow), site of subsequent biopsy. (B) Axial contrast-enhanced CT of the abdomen demonstrating irregular gastric wall thickening, ascites, and omental/peritoneal nodularity suggestive of carcinomatosis. (C) Cytomorphology of the ascitic fluid reveals the presence of loose and clustered malignant cells with a high nuclear-to-cytoplasmic ratio and prominent nucleoli, as well as abnormal mitotic figures consistent with adenocarcinoma. (D) Gastric antrum biopsy showing infiltrative atypical glandular structures with desmoplastic stromal reaction, diagnostic of poorly differentiated adenocarcinoma.
Disclosures: Julio Vega-Torres indicated no relevant financial relationships. Adrian Chico-Moya indicated no relevant financial relationships. Jose Martin-Ortiz indicated no relevant financial relationships.
Julio D. Vega-Torres, MD, PhD1, Adrian R. Chico-Moya, MD2, Jose Martin-Ortiz, MD, FACG2. P6400 - From Polyps to Peritoneum: Linitis Plastica Unmasked by Diffuse Carcinomatosis After a Diagnostic Odyssey, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.