University of California Davis Health Sacramento, CA
Aida Nasirishargh, MD1, Harjot Virk, MD, MPH2, Kuldeep Tagore, MD3 1University of California Davis Health, Sacramento, CA; 2Department of Interventional Radiology, University of California, Davis, Sacramento, CA; 3University of California Davis Health Graduate Medical Education, Sacramento, CA Introduction: Bedside percutaneous endoscopic gastrostomy (PEG) tube replacement in mature tracts ( >4 weeks old) are routinely done with as low as 1.3% rate of complications reported in case series. Here we present a rare case of an intraperitoneal PEG tube misplacement following routine bedside PEG tube exchange.
Case Description/
Methods: A 38-year-old male with refractory epilepsy and multiple intracranial procedures complicated by neuromediated dysphagia underwent PEG placement. A 24 French (Fr) deformable internal bolster tube was placed using the pull technique, with transillumination and indentation confirming proper positioning. The next day, he was tolerating tube feeds well and PEG was noted to be positioned appropriately. Over the next 6 months, he had 4 abdominal CTs for recurrent abdominal pain, all confirming appropriate tube position without complications.
Six months post-placement, GI was consulted for exchanging the mature PEG. The external bumper exhibited no erythema or leakage, and the tube was easily removed with gentle traction. A 24 Fr MIC balloon tube was inserted and flushed with 25 cc water. The patient developed abdominal pain immediately which prompted withholding tube use and a gastrografin study revealed intraperitoneal contrast extravasation. Exploratory laparotomy confirmed tube misplacement through the established tract at the level of the abdominal wall. Pre-existing tract was surgically closed and a new tube was placed. Peritoneal fluid culture grew candida albicans. About 10 days later, his clinical course was further complicated by acute cholecystitis requiring biliary drain placement.
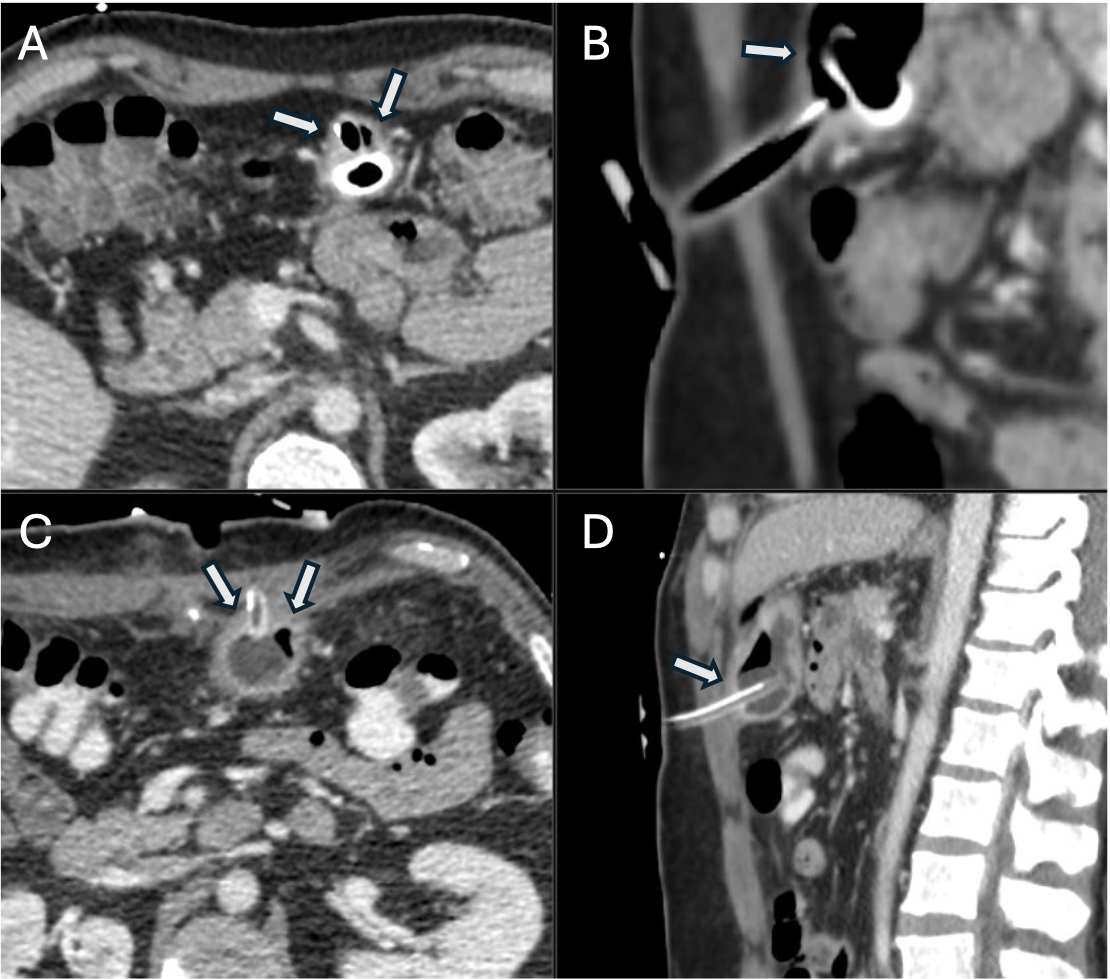
Retrospective review of the prior CT images with Radiology identified a fat layer between the gastric and abdominal walls, potentially preventing tract maturation. Bedside replacement of the tube may have resulted in false tracking into the peritoneum through the mesenteric fat (figure 1). Also, once the bumper that was pulling the stomach anteriorly was removed, the decompressed stomach may have moved away from the abdominal wall, increasing the risk of tube misplacement. Discussion: This case serves as an important reminder that “mature” PEG tracts may not guarantee safe bedside exchanges. Although rarely, anatomical variations and incomplete tract formation can predispose to serious complications. Clinical vigilance and thorough imaging review are essential to prevent adverse outcomes.
Figure: Figure 1. Contrast-enhanced computed tomography scans are shown of the endoscopically placed gastrostomy tube in axial (A) and sagittal (B) planes. The gastric wall (white arrows) is clearly seen not apposed to the abdominal wall and peritoneum and there is a layer of mesenteric fat between the gastric and abdominal wall. The subsequent surgically placed gastrostomy tube shows appropriate gastropexy and gastric wall apposition to the abdominal wall (white arrows) in axial (C) and sagittal (D) planes.
Disclosures: Aida Nasirishargh indicated no relevant financial relationships. Harjot Virk indicated no relevant financial relationships. Kuldeep Tagore indicated no relevant financial relationships.
Aida Nasirishargh, MD1, Harjot Virk, MD, MPH2, Kuldeep Tagore, MD3. P6360 - Intraperitoneal Misplacement of a PEG Tube After Routine Bedside Exchange, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.