Mariela Trejo, MD1, Simone Jarrett, MD2, Renee Williams, MD, MHPE, FACG1 1NYU Grossman School of Medicine, New York, NY; 2NYU Grossman School of Medicine, Division of Gastroenterology and Hepatology, New York, NY Introduction: Methotrexate (MTX) has various mechanisms of action, ranging from immunosuppression to folate anti-metabolism, making it suitable for the treatment of many conditions. Gastrointestinal (GI) side effects are well known due to the drug’s target towards rapidly dividing cells. Here, we present a case of a gastro-enteric fistula thought to be secondary to a MTX-induced gastric ulcer.
Case Description/
Methods: A 73-year-old female with a past medical history of GERD, rheumatoid arthritis on MTX and abatacept, Grave’s disease post thyroidectomy, and chronic kidney disease presented with presyncope, one week of coffee ground emesis and melena, two days of hematemesis, and one month of oral ulcers. She reported inadvertently taking her prescribed 25mg of MTX daily rather than weekly for the last month. On arrival, she was hemodynamically stable but intermittently hypotensive. Labs demonstrated a hemoglobin of 4.7 and leukocytosis to 42.4. CT angiography was non-diagnostic for bleeding. Initial upper endoscopy at an outside facility reported a fungating mass in the center of a large gastric ulcer. Biopsies revealed chronic inactive gastritis with focal necro-inflammatory debris suggestive of an ulcer, negative for intestinal metaplasia and H. pylori. Her hospital course was complicated by bleeding after initiation of anticoagulation, requiring pressors in the ICU. Interval endoscopy showed a clean based ulcer on the incisura measuring 8cm in diameter with an area of protruding small bowel, previously thought to be a mass, in the center of the ulcer bed. The endoscope was advanced through this area confirming a gastro-enteric fistula. MTX and abatacept were held and she was started on a high dose proton pump inhibitor with no further bleeding. After a multidisciplinary discussion with the surgical team, she was ultimately discharged with plans for repeat interval endoscopy to evaluate for healing.
Discussion: While stomatitis and GI distress are more recognized side effects of MTX, this case highlights an example of a life-threatening complication that can arise in the setting of MTX toxicity involving the GI tract. Gastro-enteric fistulas are exceedingly uncommon and often require surgical intervention for repair, however conservative management with proton pump inhibitors for healing can be initially considered in certain cases. This case demonstrates the importance of medication reconciliation and patient education with the use of immunosuppressive agents.
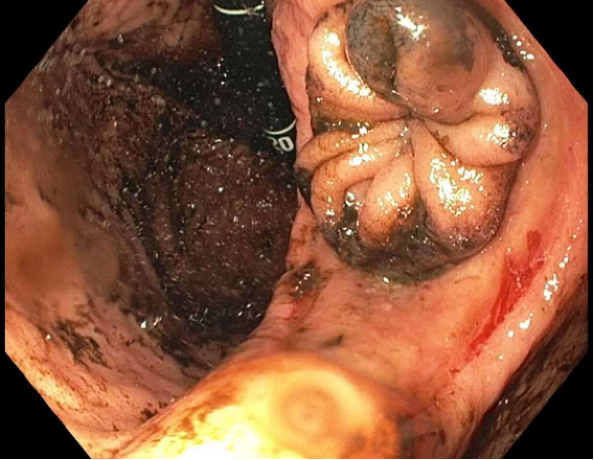
Figure: Incisura of the stomach with a portion of small bowel protruding through the gastric ulcer.
Disclosures: Mariela Trejo indicated no relevant financial relationships. Simone Jarrett indicated no relevant financial relationships. Renee Williams indicated no relevant financial relationships.
Mariela Trejo, MD1, Simone Jarrett, MD2, Renee Williams, MD, MHPE, FACG1. P6339 - Methotrexate-Induced Gastric Ulcer and Subsequent Gastro-Enteric Fistula: A Rare Complication, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")