Rochester Regional Health, Unity Hospital Rochester, NY
Marina Takawy, MD1, Tausif Syed, MD2, Mostafa Najim, MBBS3, Richard Alweis, MD4, Jason Gutman, MD5 1Rochester Regional Health, Unity Hospital, Rochester, NY; 2Rochester General Hospital, Rochester, NY; 3Unity Hospital - Rochester Regional Health, Rochester, NY; 4Rochester Regional Health, Rochester, NY; 5rochester general hospital, Rochester, NY Introduction: Post-cholecystectomy clip migration (PCCM) is a rare complication that can occur years after cholecystectomy. While most cases present within two years, delayed presentations underscore the importance of considering PCCM in differential diagnoses even decades post-surgery. Clinical presentation often mimics choledocholithiasis, leading to misdiagnosis and delayed treatment. Although exceedingly rare, spontaneous passage of the clip has been reported in literature.
Case Description/
Methods: An 85-year-old female with a history of cholecystectomy in 2005 presented to the Emergency Department with a 30-minute episode of severe epigastric pain and nausea. On presentation, she was afebrile but later developed chills, rigors, and bilious emesis. Physical examination revealed right upper quadrant and epigastric tenderness. Laboratory results showed elevated liver enzymes (AST 218 U/L, ALT 140 U/L, alkaline phosphatase 144 U/L) but normal total bilirubin and white cell count. A contrast-enhanced computed tomography (CT) scan revealed a dilated common bile duct (CBD) measuring 1.5 cm, with a hyperdense clip-like structure in the distal CBD. A follow-up magnetic resonance cholangiopancreatography (MRCP) demonstrated biliary ductal dilatation but no clip. A repeat CT three days later found the clip in the cecum, with resolving CBD dilation. This was accompanied by clinical improvement and normalization of liver enzymes. Conservative management was pursued, allowing the clip to pass naturally without further interventions. Discussion: Post cholecystectomy clip migration is an uncommon but significant complication. Early migration is often attributed to procedural factors. Late migration is believed to result from chronic inflammatory processes induced by the clip or a foreign body response. The migrated clip can obstruct the CBD and serve as a nidus for stone formation, leading to complications such as cholangitis. Diagnosis of PCCM can be established through imaging modalities such as ultrasound, CT, or MRCP. ERCP remains the gold standard for clip retrieval.
To the best of our knowledge, only 3 cases of spontaneous passage of the clip have been reported in literature. This should be suspected when the patient demonstrates improvement in the clinical presentation and laboratory parameters, even if the clip cannot be located by imaging.
Strategies to mitigate the risk of clip migration include the use of absorbable sutures, clipless cholecystectomy techniques, limiting number of clips and precise placement.
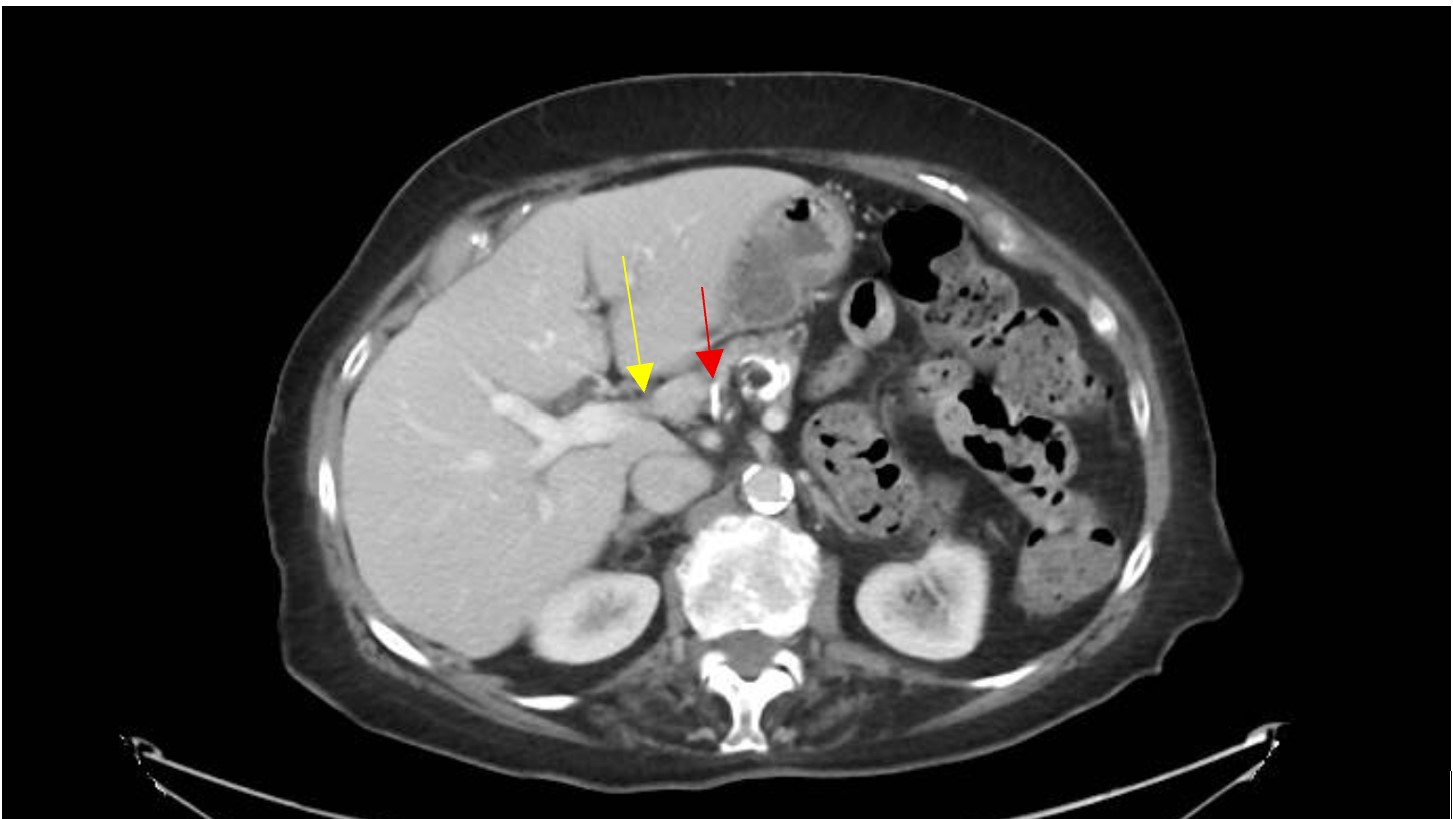
Figure: CT scan abdomen: axial view showing dilated CBD (yellow arrow) and clip migrated to the CBD (red arrow)
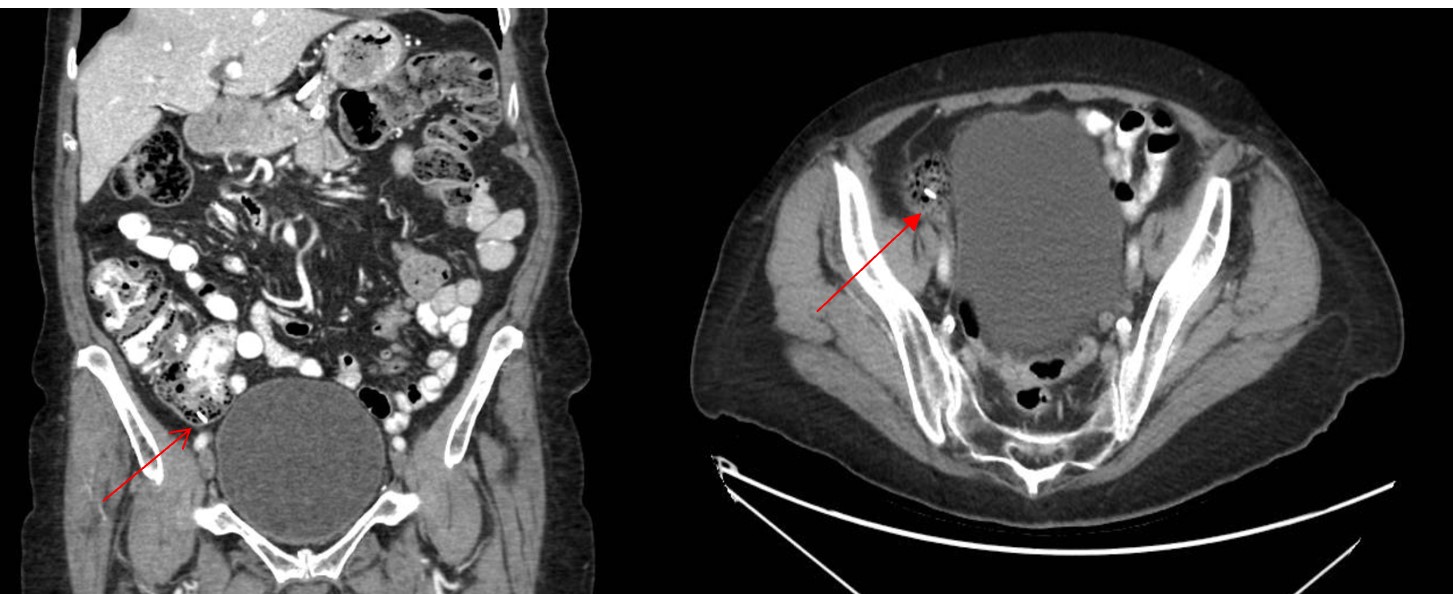
Figure: CT scan abdomen: coronal view and axial view, 3 days after presentation, Clip in cecum (red arrows).
Disclosures: Marina Takawy indicated no relevant financial relationships. Tausif Syed indicated no relevant financial relationships. Mostafa Najim indicated no relevant financial relationships. Richard Alweis indicated no relevant financial relationships. Jason Gutman indicated no relevant financial relationships.
Marina Takawy, MD1, Tausif Syed, MD2, Mostafa Najim, MBBS3, Richard Alweis, MD4, Jason Gutman, MD5. P2384 - Lost and Found: A Case of Late Post Cholecystectomy Clip Migration Causing Transient Biliary Obstruction Followed by Spontaneous Resolution, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.