Diksha Kajal, MD1, Rebecca Radcliffe, DO2, Sunny Kumar, MD3, Iryna S. Hepburn, MD, FACG1 1Florida State University, Cape Coral, FL; 2Lee Health, Cape Coral, FL; 3Wright Center for Graduate Medical Education, Scranton, PA Introduction: Large cell neuroendocrine carcinoma (LCNEC) of the colon is a very rare and aggressive subtype of colorectal cancer, often presenting at an advanced stage and posing a poor prognosis. It accounts for less than 1% of all colorectal malignancies. We present a patient with LCNEC of the right colon with metastatic disease on initial presentation.
Case Description/
Methods: A 70yo male came to the ED with generalized abdominal pain, weakness, nausea, vomiting, and dark stools for four days. On evaluation, laboratory data revealed mild anemia and CEA of 4.15. Abdominal CT showed markedly thickened colon at the hepatic flexure with surrounding inflammatory changes, enhancing hepatic lesions, and ascites concerning for metastatic malignancy. Colonoscopy revealed an ulcerated friable circumferential obstructing mass at the hepatic flexure. Patients underwent surgery for obstructive symptoms. Hystology of the mass demonstrated large cell neuroendocrine carcinoma with minor component (30%) of adenocarcinoma and signet cell morphology with metastases to regional lymph nodes and mesenteric tumor deposits. Immunohistochemical staining was positive for synaptophysin, validating neuroendocrine differentiation.
Discussion: GI neuroendocrine tumors are divided into NET grade 1, 2, and NEC based on mitotic count and Ki67 proliferation. LCNEC is more common than small cell NEC, but both are highly aggressive malignancies with poor survival rates, and the prognosis is worse than in colonic adenocarcinoma. Even localized NEC has 5- year survival of 25-40%. NEC with features of adenocarcinoma are a distinct subtype with even higher malignant potential(our patient had only a minor component of adenocarcinoma in his tumor). Most patients have stage 4 malignancy at the time of diagnosis, with a median survival of 11-12 months. Surgery is useful in obstructing or localized disease. Carbonation/etoposide is a first-line therapy, and irinotecan/fluoropyrimidines is a second-line treatment. Immunotherapy plays a minor role. Molecular profiling could help to identify new targets for therapy. As NECs have been increasing in incidence over the past several decades, more research is needed to develop means of early diagnosis and better treatment options for these aggressive neoplasms.
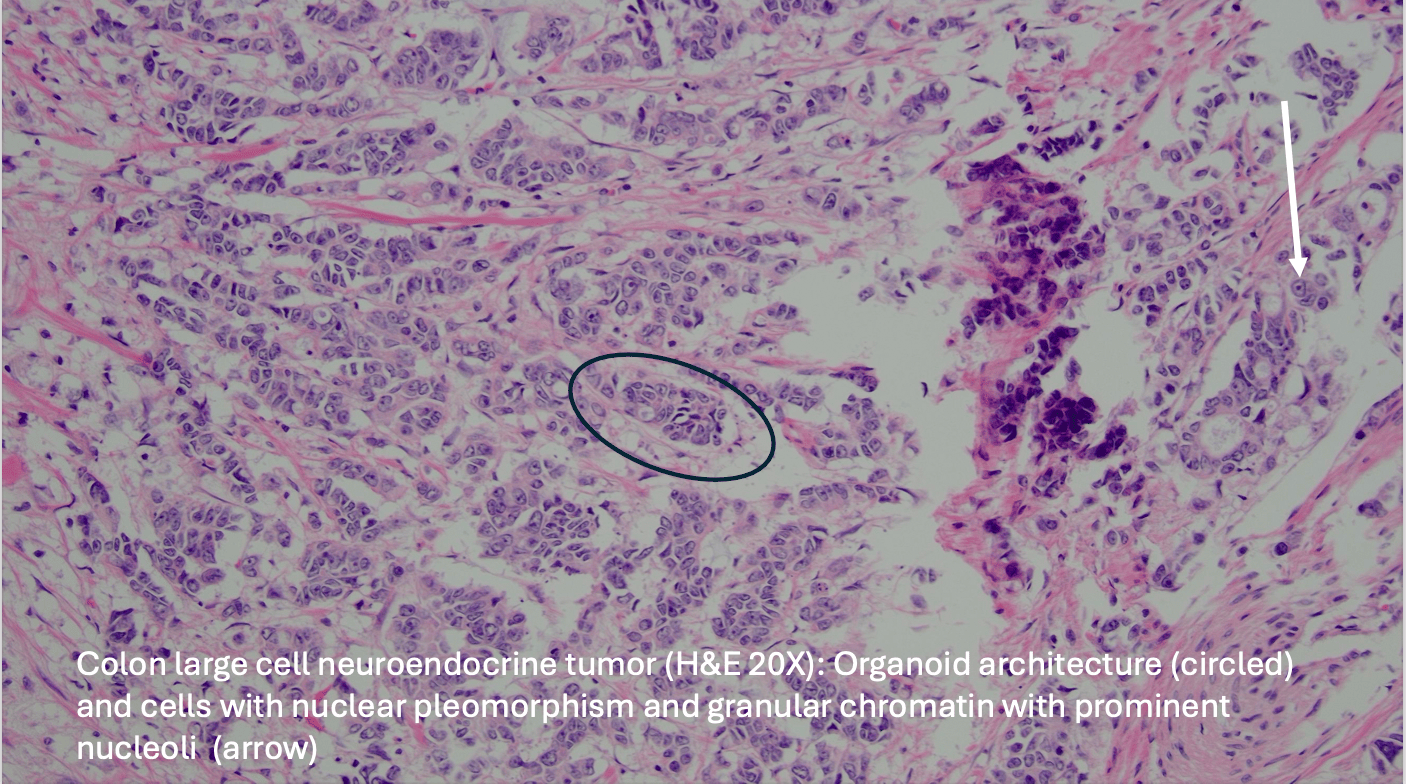
Figure: Colon large cell neuroendocrine tumor (H&E 20X): Organoid architecture (circled) and cells with nuclear pleomorphism and granular chromatin with prominent nucleoli (arrow)
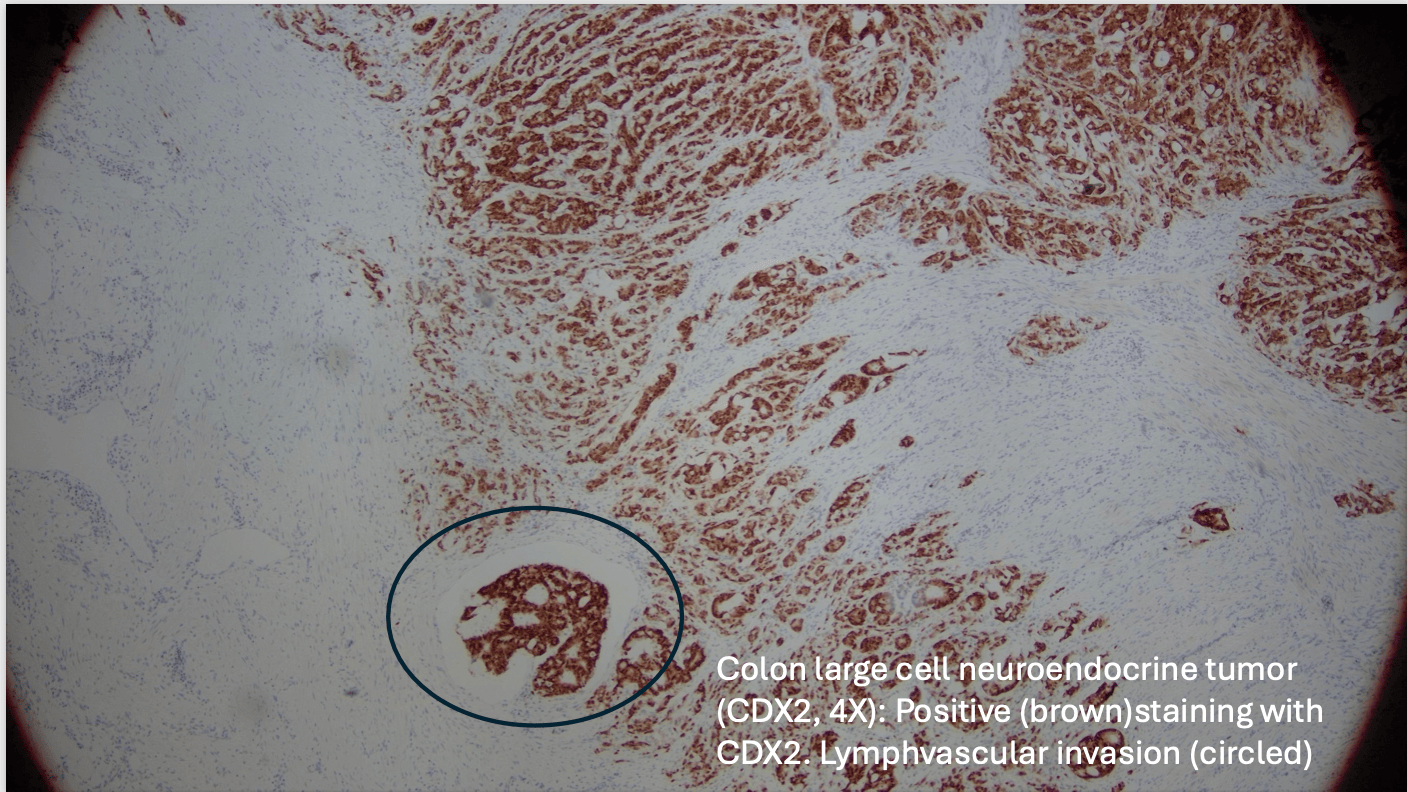
Figure: Colon large cell neuroendocrine tumor (CDX2, 4X): Positive (brown)staining with CDX2. Lymphvascular invasion (circled)
Disclosures: Diksha Kajal indicated no relevant financial relationships. Rebecca Radcliffe indicated no relevant financial relationships. Sunny Kumar indicated no relevant financial relationships. Iryna Hepburn indicated no relevant financial relationships.
Diksha Kajal, MD1, Rebecca Radcliffe, DO2, Sunny Kumar, MD3, Iryna S. Hepburn, MD, FACG1. P2489 - Large Cell Neuroendocrine Carcinoma of the Colon Presenting With Obstruction and Metastases: A Rare and Aggressive Entity, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.