Monday Poster Session
Category: Colon

Annie Shergill, MD
Larkin Community Hospital
Miami Beach, FL
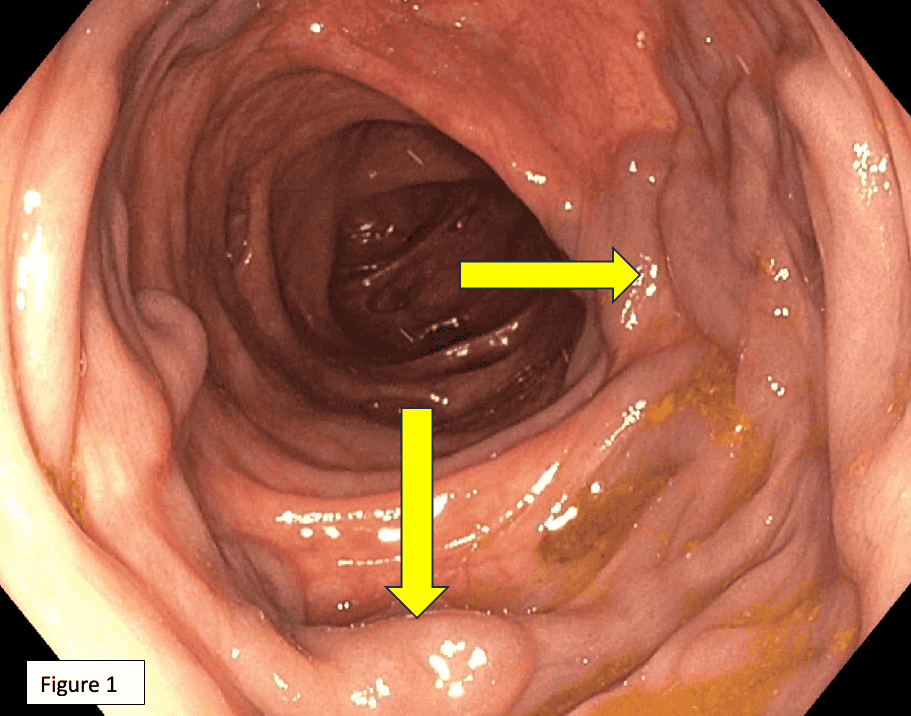
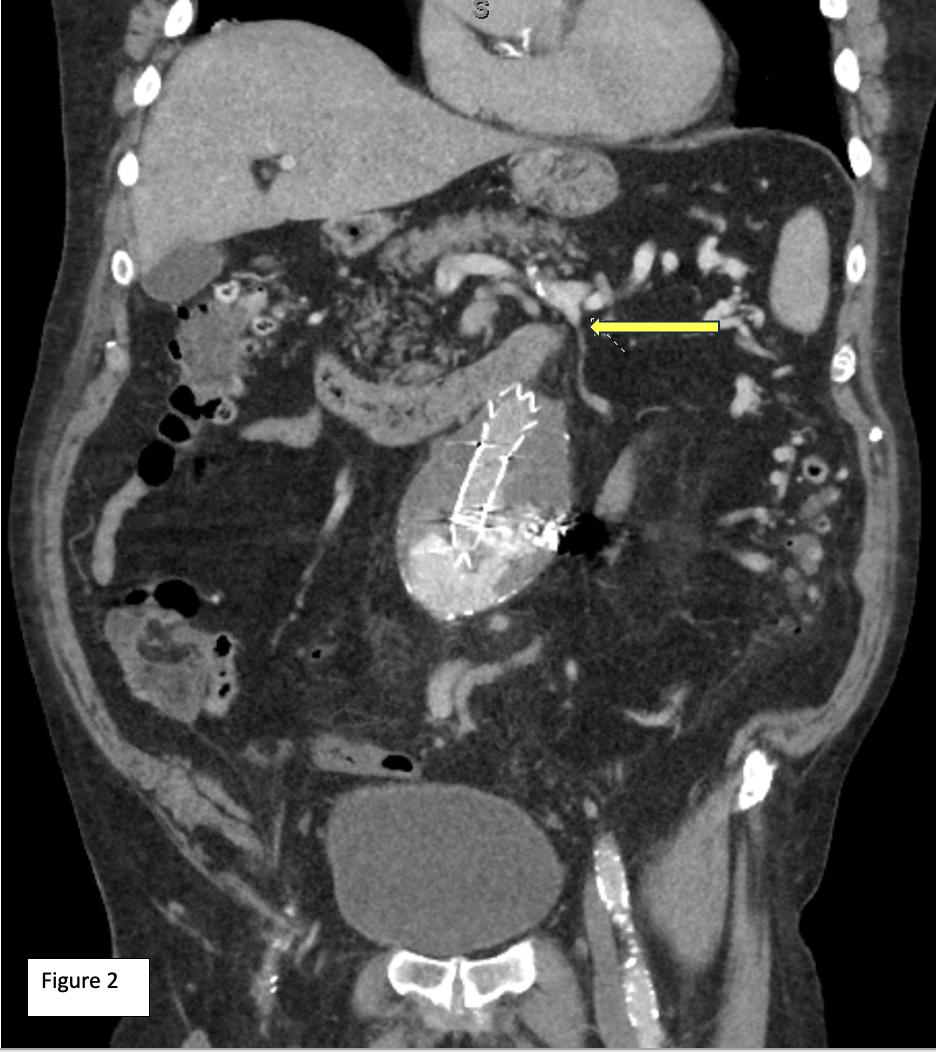
84 y/o male with history of CAD, abdominal aortic aneurysm s/p endovascular repair presented with rectal bleeding. Patient was hemodynamically stable. Labs showed a low Hb of 12.8. Colonoscopy showed mild pan diverticulosis & significantly enlarged veins noted at 50 cm around the splenic flexure (Fig 1). CT abdomen & pelvis with IV contrast showed superior mesenteric vein (SMV) collaterals & varices along the transverse & descending colon which drained into splenic flexure vein. This drained into proximal portion of the IMV (Fig 2) which then drained into the splenic vein and not directly into inferior vena cava (IVC). This caused congestion in left colonic venous drainage & variceal formation. Liver was normal, no imaging or clinical evidence of cirrhosis or PHTN.
EV are defined as dilated portosystemic veins located in sites other than the GE area. While there's a paucity of data, about 17 % of EV are found in duodenum, 14 % in colon & 8% in rectum. Most cases of EV are due to PHTN, congenital anomalous portosystemic anastomosis or related to thrombosis. EV may present with hematemesis, rectal bleeding, hematuria, or hemobilia. Endoscopic evaluation with EGD &/or colonoscopy should be pursued. IV contrast enhanced CT, double balloon or push enteroscopy & video capsule endoscopy may be considered. If EV are amenable to endoscopic intervention, then endoscopic band ligation & injection sclerotherapy can be used. Our case highlights a unique clinical scenario wherein IMV varices developed due to a rare congenital anomaly- left colonic venous system draining into splenic flexure vein which subsequently drains into IMV instead of the normal drainage pattern that entails SMV joining splenic vein to form the portal vein which eventually drains into IVC. This anomalous drainage pattern results in severe congestion in left colonic venous drainage with resultant IMV varices. Variable & complex manifestations such as our case warrant a high index of clinical suspicion in order to promptly diagnose & treat EV.