Taofeek Kolade, MD1, George Koutras, MD2, Kovil Ramasamy, MD2 1CarePoint Health - Bayonne Medical Center, Bayonne, NJ; 2Bayonne Medical Center, Bayonne, NJ Introduction: Primary gastrointestinal lymphomas comprise 1–4% of all gastrointestinal malignancies, most commonly involving the stomach or small intestine. Primary colonic lymphoma is rare, accounting for only 0.2–1% of colorectal cancers. We present a case of diffuse large B-cell lymphoma (DLBCL) of the ascending colon presenting as an obstructing mass with atypical and aggressive progression.
Case Description/
Methods: A 71-year-old man with type 2 diabetes mellitus presented with one week of right lower quadrant abdominal pain and decreased bowel movements, following six months of intermittent constipation. He denied weight loss, gastrointestinal bleeding, or family history of malignancy, and had never undergone colonoscopy. Laboratory studies revealed microcytic anemia (hemoglobin 11.4 g/dL). CT imaging of the abdomen and pelvis showed an 8.9 × 7.7 cm cecal mass and a 4.8 × 3.9 cm mesenteric nodal mass. Colonoscopy revealed a large, friable, obstructing mass in the ascending colon. Biopsies confirmed DLBCL with a Ki-67 proliferation index >90%. Staging CT identified an additional mass in the pancreatic body and tail, concerning for metastatic disease. The patient was discharged with plans for outpatient chemotherapy and multidisciplinary follow-up. Four weeks later, PET/CT demonstrated widespread hypermetabolic disease involving the colon (including the rectosigmoid region), pancreas (with interval enlargement), peritoneum, and multiple lymph node basins. Discussion: Primary colonic DLBCL is a rare malignancy that can mimic colorectal adenocarcinoma. Nonspecific symptoms such as abdominal pain and altered bowel habits often delay diagnosis. The cecum is a common site due to its abundant lymphoid tissue. Diagnosis requires endoscopic biopsy, with a high Ki-67 index indicating aggressive disease behavior. While lymphatic spread is typical, pancreatic involvement is rarely reported and suggests advanced disease. Management generally involves CHOP-based chemotherapy, with surgery or radiotherapy considered in select cases. This case underscores the importance of including lymphoma in the differential diagnosis of colonic masses, particularly in older adults presenting without classic B symptoms.
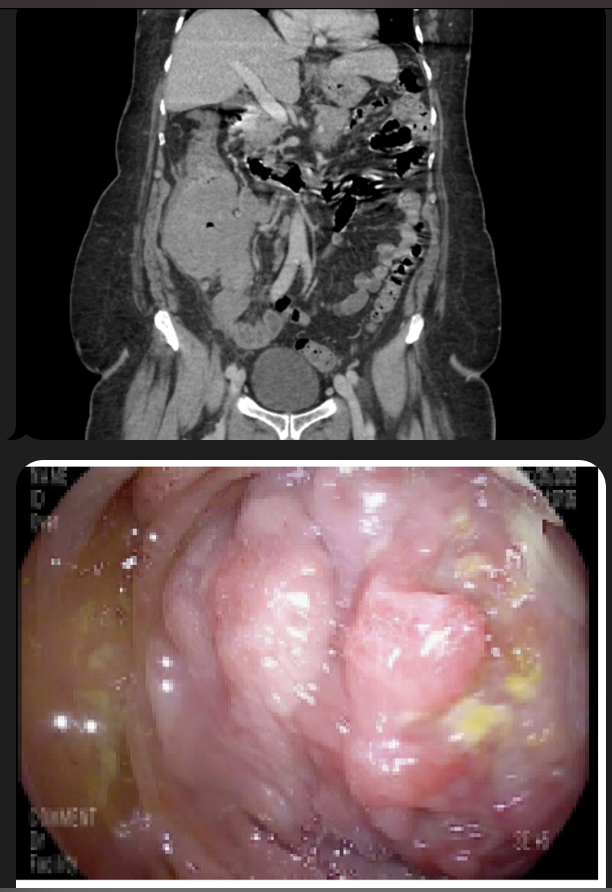
Figure: Figure I. (Top) CT abdomen/Pelvis- large mass in the area of the cecum/ileocecal valve/terminal ileum measuring 8.9 x 7.6 cm axial dimension. There is an adjacent right lower quadrant mesenteric nodal mass measuring 4.8 x 3.9 cm. (Bottom) Seen on colonoscopy- Fungating, friable and sessile mass almost completely obstructing the the ascending colon.
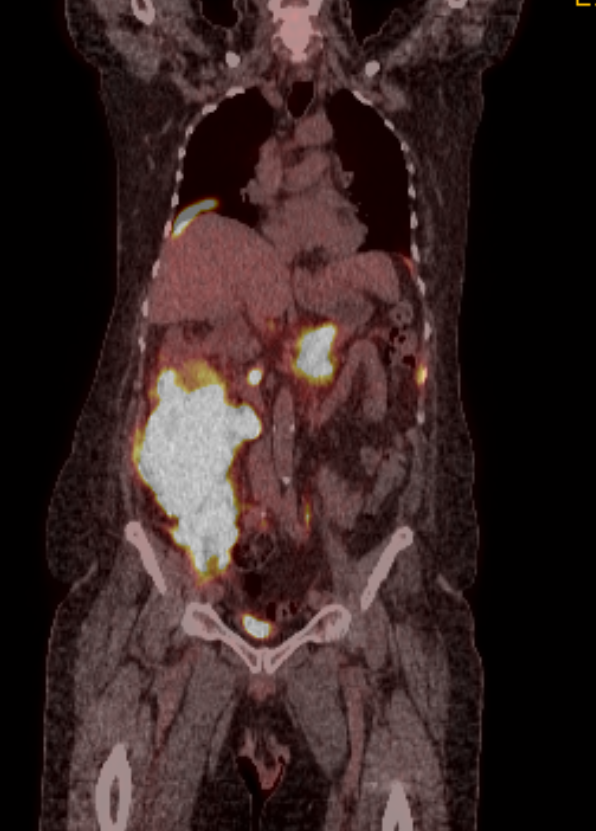
Figure: Figure II. Pet/ CT. Large mass centered at the cecum and ascending colon demonstrates significant radiotracer uptake. Uptake also noted in the pancreatic tail/body and rectosigmoid region suspicious for metastatic behavior of primary colon mass
Disclosures: Taofeek Kolade indicated no relevant financial relationships. George Koutras indicated no relevant financial relationships. Kovil Ramasamy indicated no relevant financial relationships.
Taofeek Kolade, MD1, George Koutras, MD2, Kovil Ramasamy, MD2. P2559 - Rare Colonic Diffuse Large B-Cell Lymphoma With Aggressive Progression, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.