Hospital of the University of Pennsylvania Philadelphia, PA
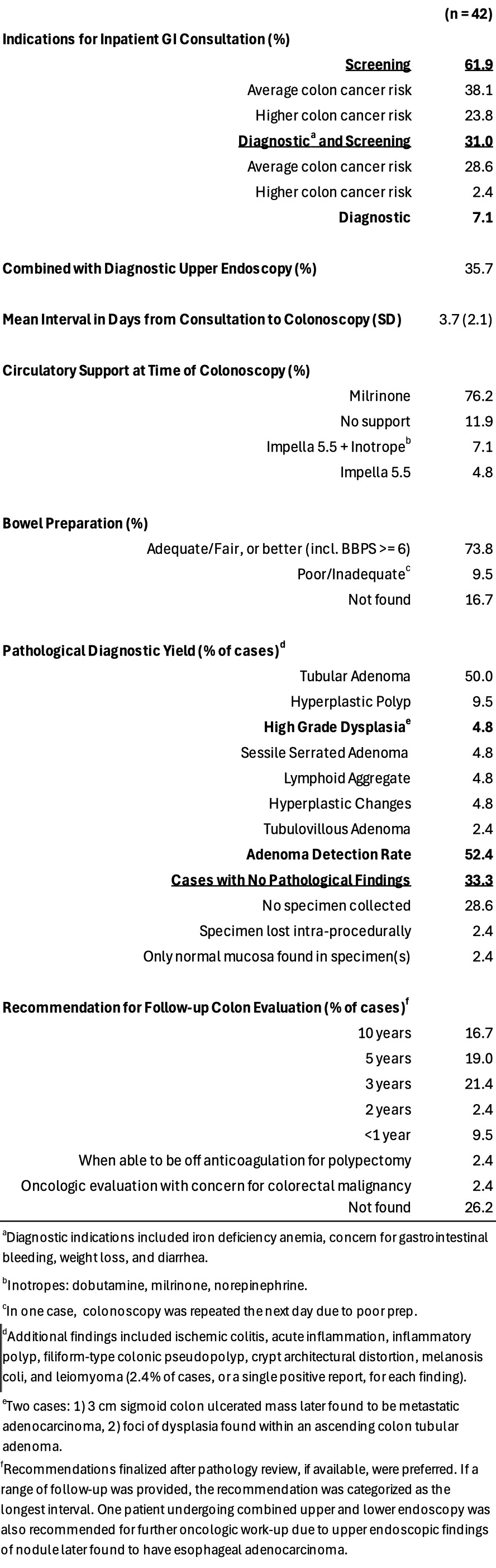
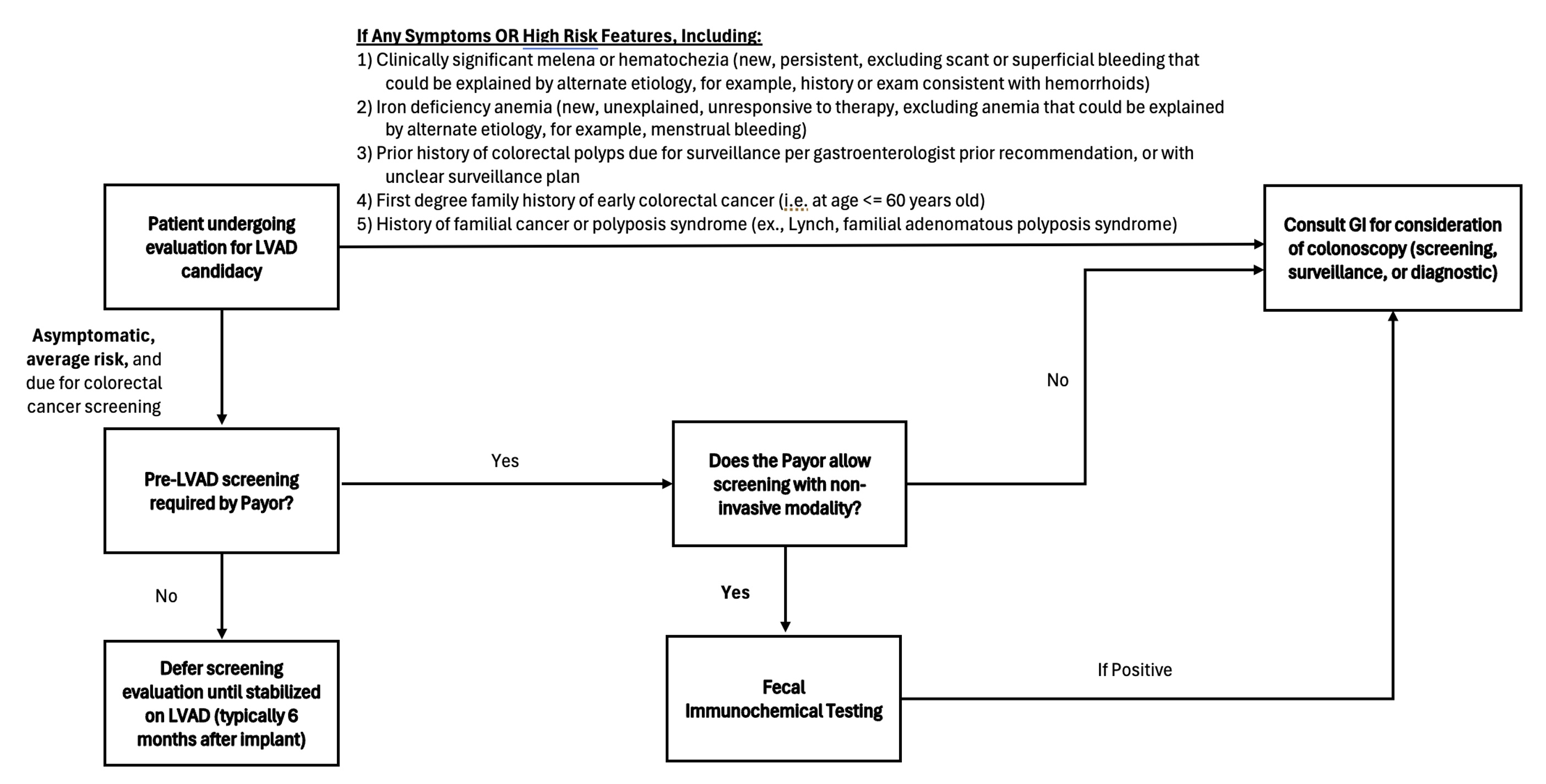
Farees Saqlain, MD, Shivan Mehta, MD, MBA, Himabindu Vidula, MD, MS, Ragunath Appasamy, MD, PhD Hospital of the University of Pennsylvania, Philadelphia, PA Introduction: Evidence supporting routine colonoscopy in evaluations for left ventricular assist device (LVAD) candidacy remains limited. In practice, guidelines and payor requirements for colorectal cancer screening (CRC) prior to organ transplant have been adapted for use in LVAD evaluations. Consultations for inpatient colonoscopy for CRC screening or to rule out possible contributors to post-implant gastrointestinal bleeding for patients under evaluation for LVAD are common and often challenging given procedural risk. Methods: We provide descriptive statistics from a 5 year cohort of patients who underwent LVAD implant at a large academic medical center (n=180, 2019-2024). For patients who underwent inpatient colonoscopy at our center prior to implant (n=42), we explored circumstances of gastroenterology consultation and diagnostic yield. Results: Median age at implant was 59 (SD=12). By time of implant, 50.6% of patients had updated colorectal cancer screening evaluations, while 20.6% did not (13.9% not indicated for screening; 15% excluded). Only 5.6% of the cohort was screened exclusively with non-invasive modalities. 42 patients underwent inpatient colonoscopy at our center prior to implant, with the most common indication being average risk screening (38.1%; Figure 1). Mean interval from consult to colonoscopy was 3.7 days (SD=2.1). Diagnostic yield of inpatient colonoscopies was notable for a 52.4% adenoma detection rate. Two cases of high-grade dysplasia were discovered, with one patient eventually diagnosed with metastatic adenocarcinoma. No cases revealed lesions with recent or active bleeding, except for a single case revealing clot associated with an anal fissure that was not intervened on. Discussion: Pre-LVAD colonoscopy of 42 patients resulted in one diagnosis of adenocarcinoma and no discovered sources of intervenable bleeding. Potential risks of inpatient colonoscopy include prolonged admission and complications of bowel prep, anesthesia, or post-procedural bleeding. Our findings suggest it is unlikely that routine CRC screening prior to implant will change clinical management leading up to implant. We suggest deferring screening until patients are stable post-LVAD, or at least considering stool-based screening for eligible patients instead of colonoscopy. Our center plans to implement a clinical pathway with this rationale, with discussion ongoing to extend a similar approach to solid organ transplant where applicable (Figure 2).
Figure: Figure 1. Clinical Setting and Diagnostic Yield of Inpatient Colonoscopies for Patients Prior to LVAD Implant
Figure: Figure 2. Suggested Pathway for Colorectal Cancer Screening for Patients Undergoing LVAD Evaluation
Disclosures: Farees Saqlain indicated no relevant financial relationships. Shivan Mehta indicated no relevant financial relationships. Himabindu Vidula indicated no relevant financial relationships. Ragunath Appasamy indicated no relevant financial relationships.
Farees Saqlain, MD, Shivan Mehta, MD, MBA, Himabindu Vidula, MD, MS, Ragunath Appasamy, MD, PhD. P2665 - Diagnostic Yield of Inpatient Colonoscopies for Patients Undergoing Evaluation Prior to Left Ventricular Assist Device Implantation, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")