University of Pennsylvania Health System CHICAGO, IL
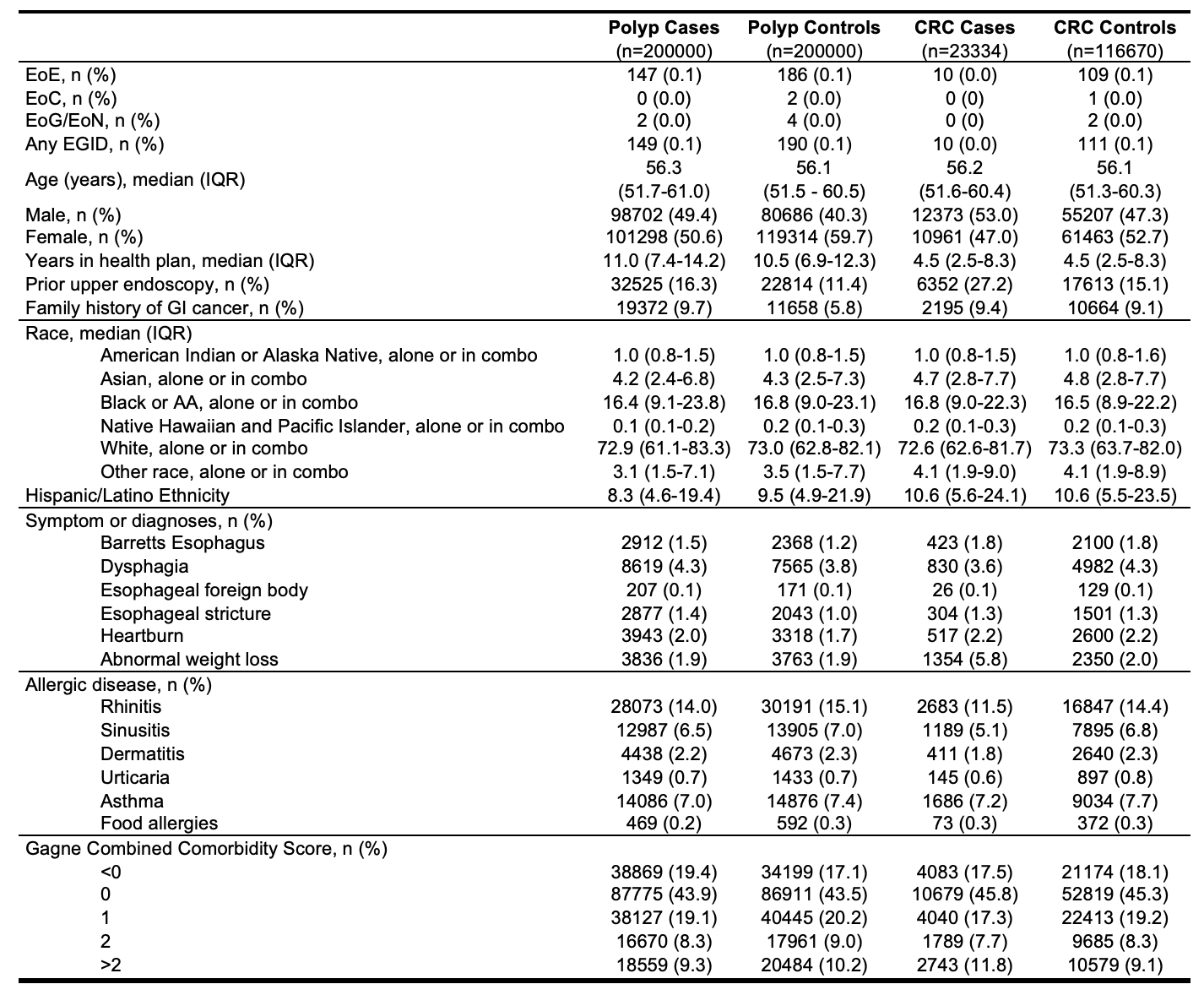
Corey J. Ketchem, MD1, Evan S. Dellon, MD, MPH2, Natasha Albaneze, MPH3 1University of Pennsylvania Health System, Philadelphia, PA; 2Center for Esophageal Diseases and Swallowing, University of North Carolina School of Medicine, Chapel Hill, NC; 3University of North Carolina at Chapel Hill, Chapel Hill, NC Introduction: Allergic inflammation may protect against cancer development, but the relationship of eosinophilic gastrointestinal diseases (EGIDs) and eosinophilic esophagitis (EoE) to colorectal neoplasia is unclear. We aimed to evaluate the association between EGIDs and the risk of colon polyps and colorectal cancer (CRC) diagnosis among average-risk adults undergoing screening colonoscopy. Methods: Using administrative claims data, we conducted two matched case-control studies among individuals aged 45-64 years. For the polyp analysis, 200,000 individuals with a polyp diagnosis on the day of screening colonoscopy were matched 1:1 to controls without polyp codes. For the CRC analysis, 23,334 individuals with a colon cancer diagnosis within one year of colonoscopy were matched 1:5 to controls without CRC in one year. We matched on age, colonoscopy date (±3 months), and time in health plan. All participants had ≥1 year of claims pre-colonoscopy, and no prior history of polyps, CRC, or inflammatory bowel disease. EGID diagnoses were identified using as having at least two primary diagnostic codes for EoE or non-EoE EGIDs (e.g., eosinophilic colitis, gastritis/enteritis) ≥ 30 days apart pre-colonoscopy. Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated, adjusted for sex and age where appropriate, using EGID as exposure and colorectal neoplasia as outcome. Results: EGID diagnoses were seen in 149 polyp and 10 CRC cases, compared with 186 and 109 controls, respectively (Table 1). EoE was most common. Demographic and clinical variables were balanced after matching. In the polyp analysis, history of EoE was associated with lower odds of polyp diagnosis in both unadjusted (OR 0.79, 95% CI: 0.63-0.98) and adjusted models (aOR 0.75, 95% CI: 0.60-0.93). Similarly, any EGID diagnosis was associated with reduced odds of polyps (OR 0.78, 95% CI: 0.63-0.97; aOR 0.74, 95% CI: 0.60-0.92) (Table 2). In the CRC analysis, EoE was associated with significantly lower odds of CRC in both unadjusted (OR 0.46, 95% CI: 0.24-0.88) and adjusted models (aOR 0.44, 95% CI: 0.23-0.85). Findings were similar for any EGID (OR 0.45, 95% CI: 0.24-0.86; a OR 0.44, 95% CI: 0.23-0.83). Discussion: In this large case-control study, EGIDs, particularly EoE, were associated with significantly lower odds of both colorectal polyps and cancer diagnoses in average-risk adults undergoing screening colonoscopy. Further research is needed to explore this relationship and underlying mechanisms.
Figure: Table 1. Distribution of key demographic and clinical variables across cases and controls for both polyp and colorectal cancer analyses.
Figure: Table 2. Odds ratios for outcome of colon polyp or colorectal cancer diagnostic code with exposure of EGID diagnosis.
Corey J. Ketchem, MD1, Evan S. Dellon, MD, MPH2, Natasha Albaneze, MPH3. P2741 - Eosinophilic Gastrointestinal Diseases Are Associated With a Lower Odds of Colorectal Neoplasia Diagnosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.