University of Connecticut Health Center Farmington, CT
Lucas Versland, DO1, Ismail Ghafary, MD1, Mark Versland, MD1, Susan Parker, MD2 1University of Connecticut Health Center, Farmington, CT; 2Hospital of Central Connecticut, New Britain, CT Introduction: Lymphocytic esophagitis (LE) is a rare inflammatory disorder first described in 2006. The etiology remains unclear—it may represent a unique entity or a manifestation of other diseases. LE more often affects older females and is associated with GERD, smoking, achalasia, hypothyroidism, and medications like aspirin or statins [2]. Symptoms include dysphagia, heartburn, chest discomfort, or food impaction and may also coexist with autoimmune or motility disorders [3]. Endoscopically, findings may mimic eosinophilic esophagitis (EoE), with rings, strictures, or linear furrows; however, the diagnosis of LE requires histologic confirmation [4].
Case Description/
Methods: An 89-year-old woman with a history of GERD and COPD presented with solid food dysphagia and regurgitation. She reported long-standing symptoms despite daily omeprazole. EGD revealed rings, crepe-paper mucosa, and a benign stricture—findings suggestive of EoE. However, histology ultimately revealed a different diagnosis. She underwent dilation and biopsies of the proximal and distal esophagus. Biopsies showed intraepithelial lymphocytosis without granulocytes. Immunostaining confirmed the T-cell predominance characteristic of LE, with CD3+ lymphocytes and minimal CD20+ B-cell involvement. Despite BID PPI therapy, dysphagia persisted after 12 weeks, and topical budesonide was initiated. Discussion: LE cannot be reliably distinguished from EoE based on symptoms, demographics, or endoscopic appearance. LE tends to affect older females, while EoE is more common in young males, but both may present with similar clinical features [2,5]. Histologic examination is essential for diagnosis. LE is characterized by peripapillary lymphocytosis without granulocytes [5]. Though no strict histologic thresholds exist, >20 lymphocytes/HPF is commonly used. The lymphocytes are typically CD3+, often CD4+ or CD8+, with minimal CD20+ B-cell involvement [2]. Treatment begins with PPI; non-responders may need topical steroids. Endoscopic dilation may be required for strictures. No formal LE guidelines exist; treatment often mirrors EoE protocols. This case highlights the diagnostic limitations of endoscopy alone and reinforces the essential role of biopsy in distinguishing LE from EoE to guide appropriate treatment.
Banks WD et al. Cureus. 2022;14(10):e30300.
Ravelli AM et al. J Pediatr Gastroenterol Nutr. 2017;64(6):930–6.
Cohen S et al. J Clin Gastroenterol. 2012;46(10):828–32.
Habbal M et al. Esophagus. 2019;16(2):123–32.
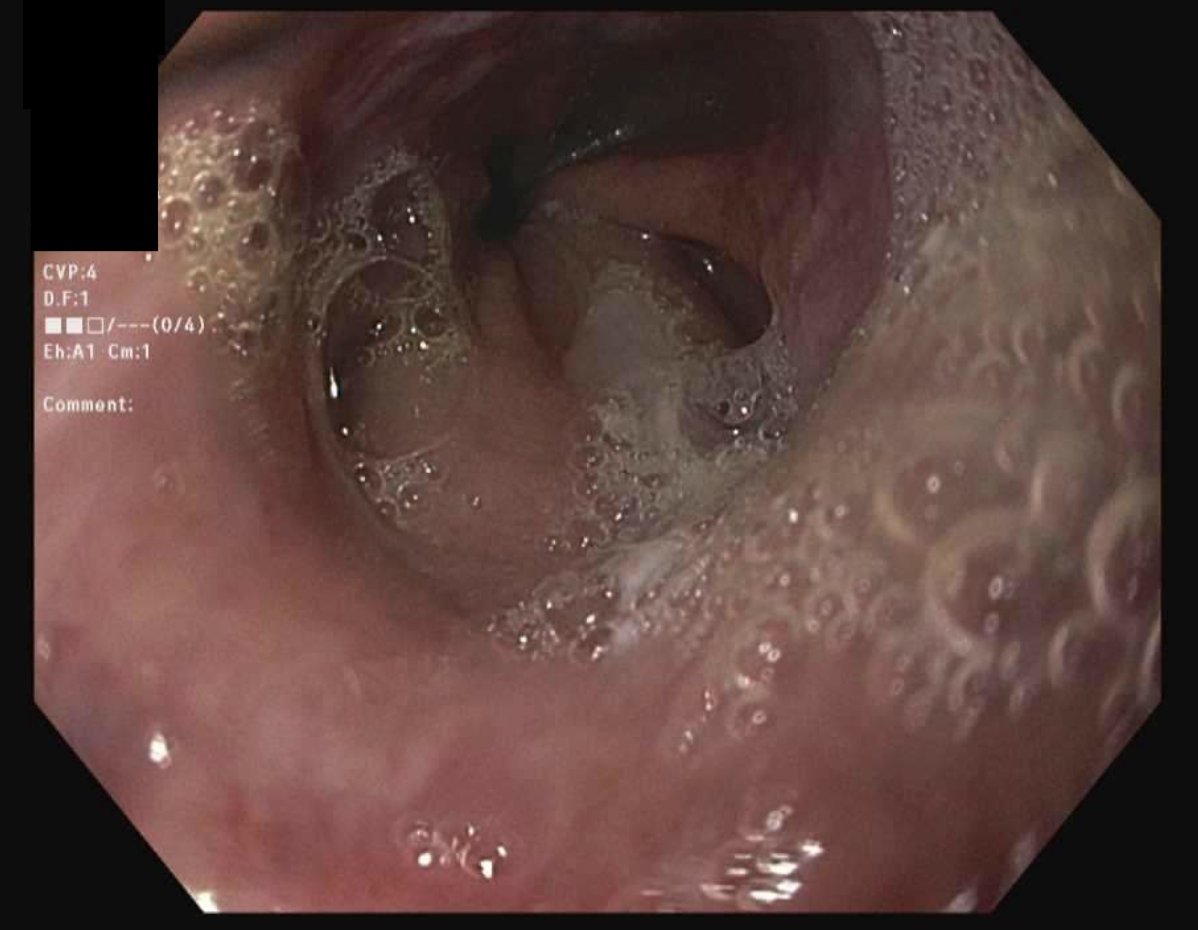
Figure: Endoscopic findings demonstrating characteristic features initially suggestive of eosinophilic esophagitis: multiple concentric rings, mucosal fragility (crepe-paper esophagus), friability, and a benign-appearing esophageal stricture.
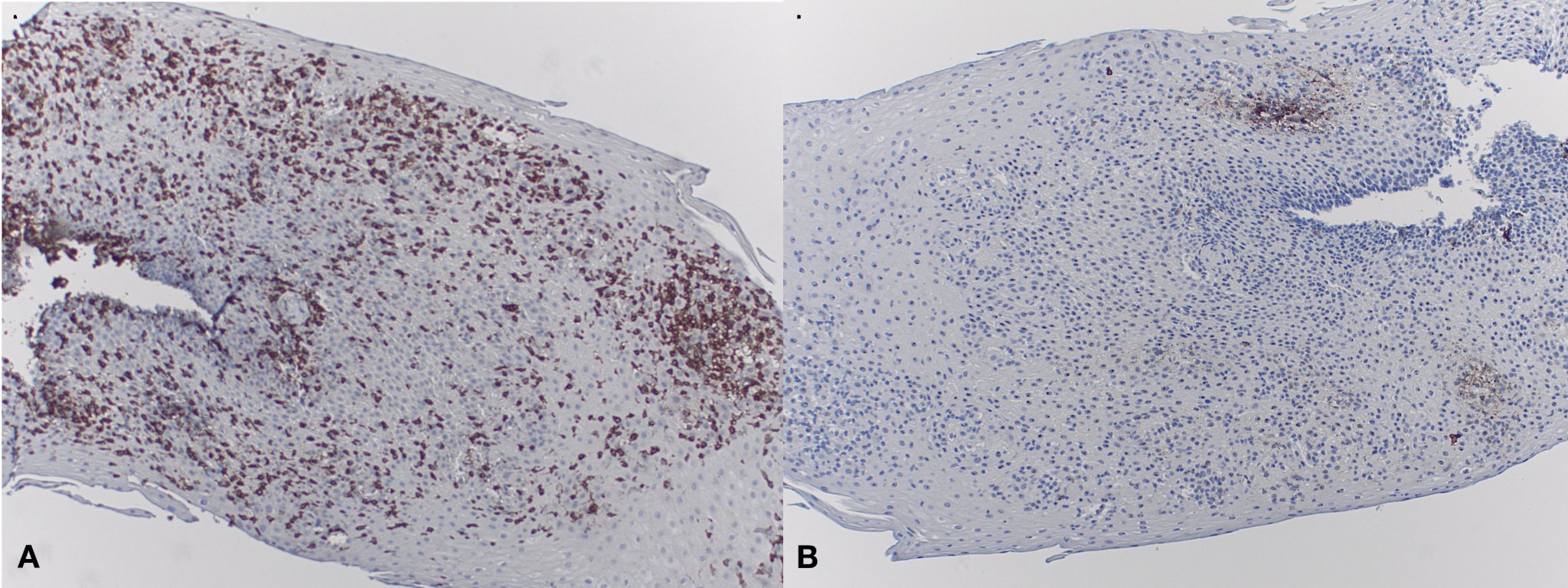
Figure: Histologic evaluation of esophageal biopsies with immunohistochemical staining: A. CD3 staining shows a dense infiltration of intraepithelial T-lymphocytes, consistent with lymphocytic esophagitis. B. CD20 staining shows minimal B-cell presence, supporting T-cell predominance.
Disclosures: Lucas Versland indicated no relevant financial relationships. Ismail Ghafary indicated no relevant financial relationships. Mark Versland indicated no relevant financial relationships. Susan Parker indicated no relevant financial relationships.
Lucas Versland, DO1, Ismail Ghafary, MD1, Mark Versland, MD1, Susan Parker, MD2. P2839 - Not All Rings Are EoE: Histologic Revelation of Lymphocytic Esophagitis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.