Saint Louis University School of Medicine Saint Louis, MO
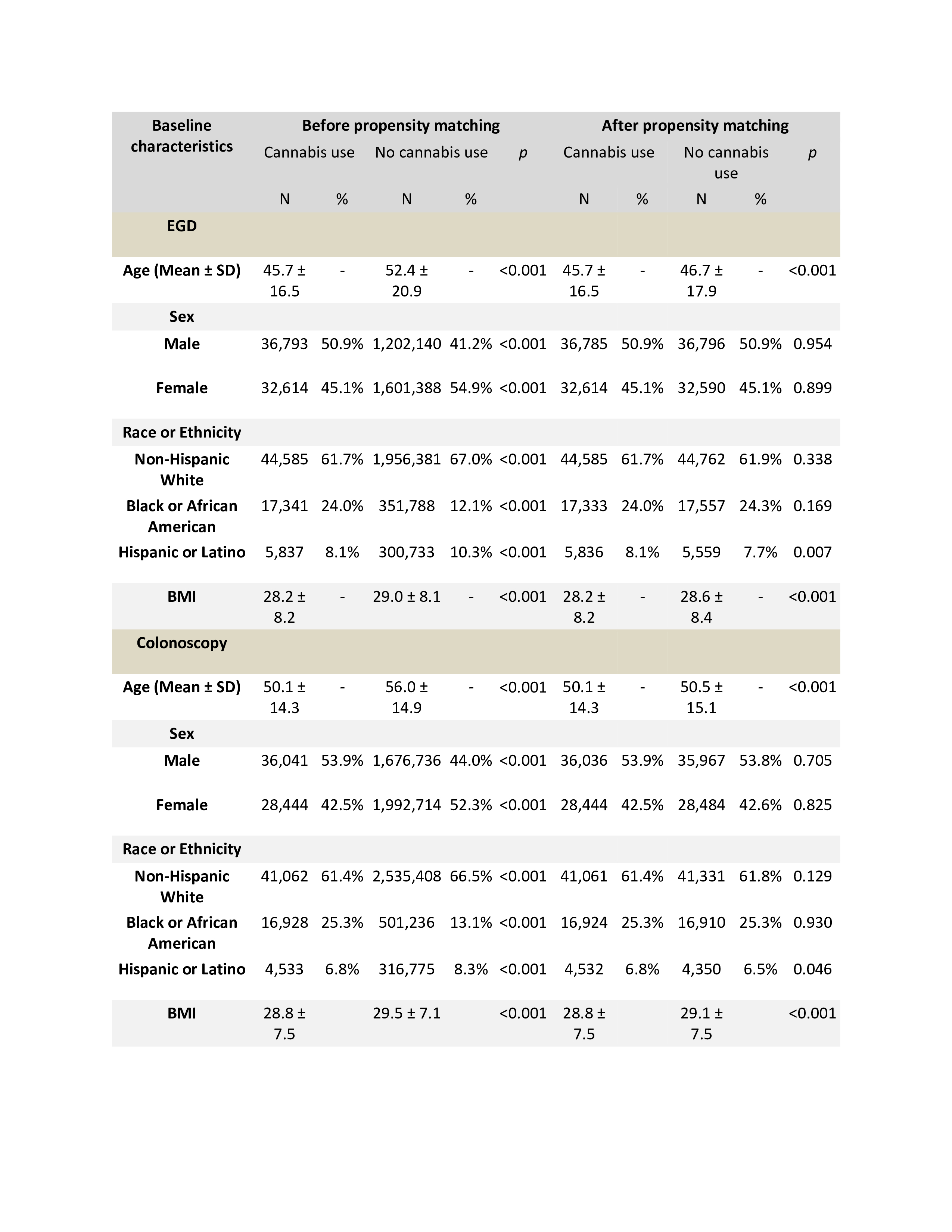
Yassine Kilani, MD1, Pradeep Yarra, MD1, Shravya R. Ginnaram, MD2, Ahmad Basil Nasir, MD1, Kym Yves Sirilan, MD3, Alfred Nelson, MD1 1Saint Louis University School of Medicine, Saint Louis, MO; 2University of Nebraska Medical Center, Omaha, NE; 3Lincoln - Weill Cornell Medical College, Bronx, NY Introduction: Despite the rising prevalence of cannabis use among patients undergoing esophagogastroduodenoscopy (EGD) and colonoscopy, there is a lack of clinical studies evaluating its impact on post-endoscopy complications remains poorly understood. This study aims to address this knowledge gap by evaluating the incidence of complications in patients undergoing EGD or colonoscopy using cannabis compared to those who are non-users. Methods: We conducted a retrospective cohort study in the United States using the TriNetX database to identify adults (≥18 years) undergoing EGD or colonoscopy and using cannabis. This cohort was matched with patients undergoing EGD or colonoscopy and not using cannabis using 1:1 propensity score matching. Outcomes were the incidence of perforation, aspiration pneumonia, and emergency intubation within 10 days after EGD/colonoscopy. With censoring applied, Kaplan-Meier analysis with hazard ratios (HRs) and 95% CIs was used to compare time-to-event rates at daily time intervals. Results: A total of 68,003 patients undergoing EGD/colonoscopy and using cannabis were identified and propensity matched with 3,983,392 non-users, resulting in 66,894 matched pairs. Patients treated with cannabis were younger, and more likely non-Hispanic Blacks, with higher rates of obesity as compared to controls (Table 1). After matching, patients undergoing EGD or colonoscopy and using cannabis had no significant differences in the risk of perforation (EGD: 0.04% vs. 0.04%; adjusted hazard ratio (aHR) = 0.93, 95% CI: 0.56–1.55; colonoscopy: 0.04% vs. 0.04%; aHR = 1.11, 95% CI: 0.65–1.89), aspiration pneumonia (EGD: 0.18% vs. 0.16%; aHR = 1.12, 95% CI: 0.86–1.44; colonoscopy: 0.04% vs. 0.04%; aHR = 1.05, 95% CI: 0.62–1.78), and emergency intubation (EGD: 0.04% vs. 0.04%; aHR = 1.36, 95% CI: 1.11–1.67; colonoscopy: 0.06% vs. 0.07%; aHR = 0.85, 95% CI: 0.55–1.31) at 10 days follow-up (Table 2). Discussion: Our findings provide real-world evidence that cannabis use in patients undergoing EGD or colonoscopy does not significantly increase or reduce the risk of complications compared to non-users. These results suggest that cannabis use may not be an independent risk factor for morbidity following gastrointestinal endoscopy. However, further prospective studies are needed to clarify its role in procedural outcomes and potential interactions with patient risk profiles.
Figure: Baseline characteristics of our study population and matching variables
Figure: Complications of endoscopic procedures
Disclosures: Yassine Kilani indicated no relevant financial relationships. Pradeep Yarra indicated no relevant financial relationships. Shravya Ginnaram indicated no relevant financial relationships. Ahmad Basil Nasir indicated no relevant financial relationships. Kym Yves Sirilan indicated no relevant financial relationships. Alfred Nelson indicated no relevant financial relationships.
Yassine Kilani, MD1, Pradeep Yarra, MD1, Shravya R. Ginnaram, MD2, Ahmad Basil Nasir, MD1, Kym Yves Sirilan, MD3, Alfred Nelson, MD1. P2984 - Cannabis Use and Procedural Outcomes of Esophagogastroduodenoscopy and Colonoscopy: A Propensity Score-Matched Analysis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.