Wright Center for Graduate Medical Education Scranton, Pennsylvania
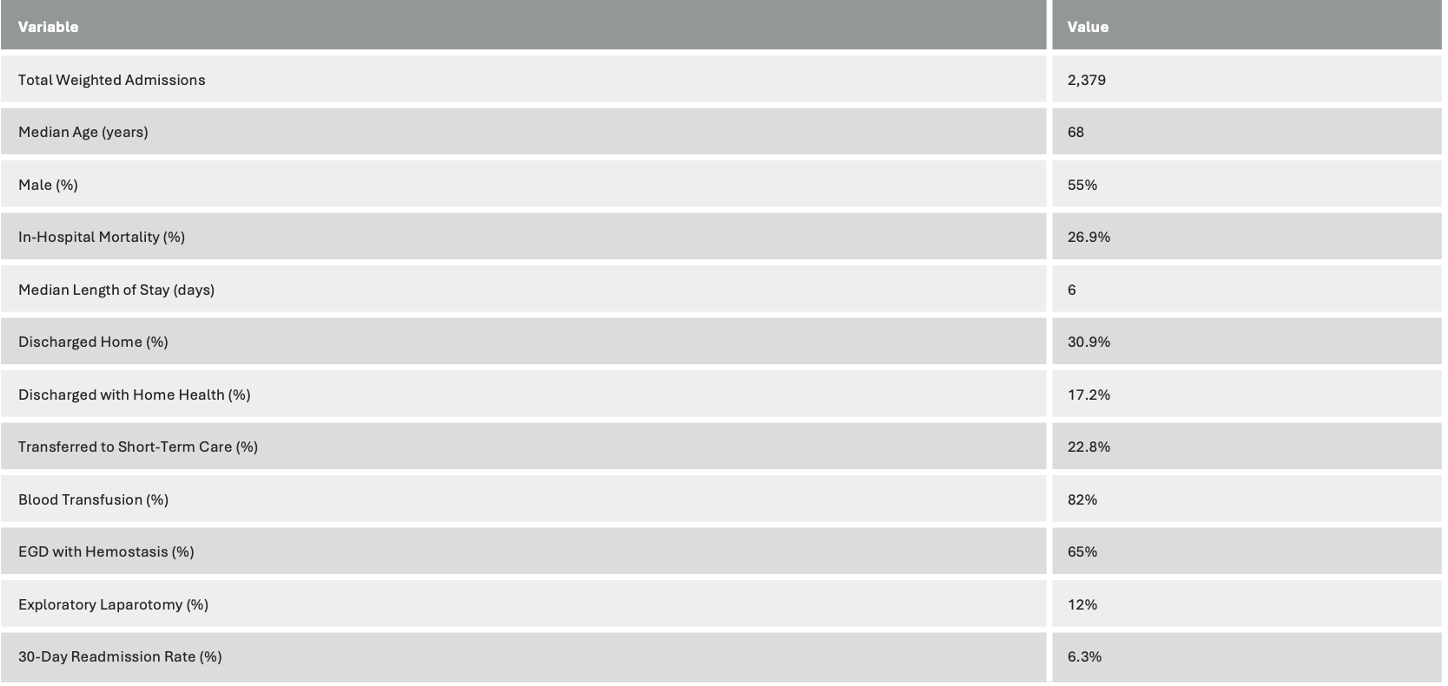
Satish Kumar Ahuja, MD1, Sunny Kumar, MD1, Ashok Kumar, MD2, Rahul Kumar, MD3, Avinash Nankani, MBBS4, Rubela Ray, MD5, Diksha Kajal, MD6, Sushrut Ingawale, MD, DNB, MBBS7, Osama Abdur Rehman, MD6, Balla Achyuth, MBBS8 1Wright Center for Graduate Medical Education, Scranton, PA; 2Ascension Saint Joseph Hospital, Chicago, IL; 3North Central Bronx Hospital, Bronx, NY; 4Dow University of Health Sciences, Karachi, Sindh, Pakistan; 5University of Wyoming, Cheyenne, WY; 6Florida State University, Cape Coral, FL; 7Quinnipiac University - Frank H Netter MD School of Medicine, Bridgeport, CT; 8Government Medical College Siddipet, Hyderabad, Telangana, India Introduction: Hemorrhagic shock due to gastrointestinal (GI) bleeding is a medical emergency with high mortality and resource utilization. We analyzed national trends in outcomes, procedures, and readmission rates using the National Readmission Database (NRD) from 2016 to 2023. Methods: Adult patients hospitalized with a primary diagnosis of hypovolemic shock and a secondary diagnosis of GI bleeding were identified from the NRD (2016–2023) using ICD-10 codes. Discharge weights were applied to generate national estimates. Outcomes included demographics, in-hospital mortality, length of stay (LOS), discharge disposition, procedures performed, and 30-day readmission rates. Results: A total of 2,379 weighted index admissions were identified from 2016–2023. Median age was 68 years, and 55% were male. The overall in-hospital mortality was 26.9%. The median LOS was 6 days. A majority (30.9%) were discharged home, 17.2% to home health care, and 22.8% to short-term acute care.
Socioeconomic data showed a higher burden among patients in the lowest income quartile (32.2%). Common procedures included blood transfusion (82%), esophagogastroduodenoscopy (EGD) with control of bleeding (65%), and exploratory laparotomy (12%). Discussion: Hemorrhagic shock due to GI bleeding carries high in-hospital mortality despite aggressive interventions. This national analysis highlights the need for improved care coordination, especially among socioeconomically disadvantaged groups. The low but notable readmission rate emphasizes the importance of structured follow-up in survivorship care and may reflect either efficient inpatient management or incomplete readmission capture in administrative datasets.
Figure: Table 1: Summary of Key Outcomes (2016–2023)
Disclosures: Satish Kumar Ahuja indicated no relevant financial relationships. Sunny Kumar indicated no relevant financial relationships. Ashok Kumar indicated no relevant financial relationships. Rahul Kumar indicated no relevant financial relationships. Avinash Nankani indicated no relevant financial relationships. Rubela Ray indicated no relevant financial relationships. Diksha Kajal indicated no relevant financial relationships. Sushrut Ingawale indicated no relevant financial relationships. Osama Abdur Rehman indicated no relevant financial relationships. Balla Achyuth indicated no relevant financial relationships.
Satish Kumar Ahuja, MD1, Sunny Kumar, MD1, Ashok Kumar, MD2, Rahul Kumar, MD3, Avinash Nankani, MBBS4, Rubela Ray, MD5, Diksha Kajal, MD6, Sushrut Ingawale, MD, DNB, MBBS7, Osama Abdur Rehman, MD6, Balla Achyuth, MBBS8. P3060 - Hemorrhagic Shock Secondary to GI Bleeding: A National Analysis of Outcomes Using the NRD (2016-2023), ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.