Shree Patel, MD, Nikita Desai, MD, Gabriela Oprea, MD, Tanvi Dhere, MD Emory University School of Medicine, Atlanta, GA Introduction: Meckel’s diverticulum (MD) can be a challenging gastrointestinal emergency. Here we report an unusual case of a jejunal MD that presented after a traumatic fall in an older patient which was successfully managed using a multi-disciplinary approach.
Case Description/
Methods: We present the case of a 66-year-old male with type 2 diabetes, hypertension, and coronary artery bypass grafting on clopidogrel who was transferred to our trauma center following a fall and acute loss of lower extremity motor and sensory function. Prior imaging revealed a burst fracture at T11 with complete spinal cord transection. Shortly after transfer, the patient experienced large-volume hematochezia resulting in hemodynamic instability.Physical exam demonstrated bilateral lower extremity paralysis, absent rectal tone, and gross blood on digital rectal exam. Labs were notable for elevated WBC 22.7 cells/L, worsening anemia (Hb 11.4 gm/dL from 12.3 gm/dL), hyperkalemia (K⁺ 6.3 mEq/L), and anion gap metabolic acidosis. CT angiography showed no active bleeding. Emergent upper endoscopy with enteroscopy was performed and revealed coffee-ground material in the stomach and extensive clot burden extending into the proximal jejunum, but no definitive source was identified. An area that was notable for pooled blood at the maximal point of insertion was marked with an endoscopic clip and India ink. Due to ongoing bleeding requiring over 10 units of packed red blood cells, the patient underwent IR guided angiography which failed to reveal the source of bleeding. An intraoperative enteroscopy was subsequently performed with the assistance of the trauma and GI teams. The procedure led to the identification of an ulcerated diverticulum with large adherent clot 5 cm distal to the tattoo. Segmental resection of the involved jejunum was performed. Pathology revealed a MD with hemorrhage, erosion, and granulation tissue. Discussion: Our case is unique for three reasons. First, the diagnosis was made after a traumatic fall injury. Reports of damage to MD have been described after blunt abdominal trauma. The potential mechanism may be due to shearing forces during the fall that may have led to overstretching and rupture of a blood vessel. Second, the case involved a 66-year-old patient. Most patients present before the age of 50. Lastly, the lesion was found in the jejunum, whereas most MD are found in the ileum. A multidisciplinary approach may be needed to manage complicated cases such as ours.
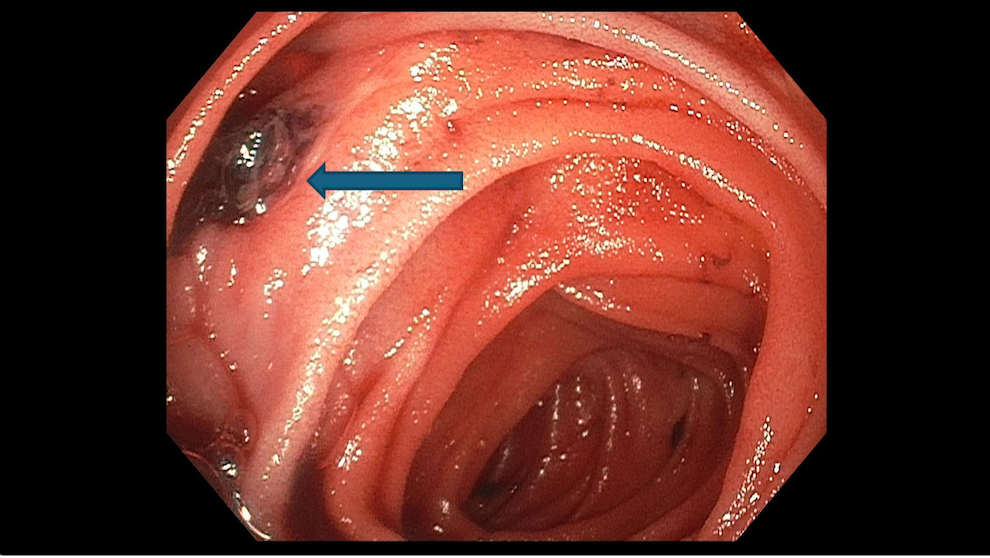
Figure: Image 1: Endoscopic image of jejunal diverticulum with ulceration and clot (arrow).
Disclosures: Shree Patel indicated no relevant financial relationships. Nikita Desai indicated no relevant financial relationships. Gabriela Oprea indicated no relevant financial relationships. Tanvi Dhere indicated no relevant financial relationships.
Shree Patel, MD, Nikita Desai, MD, Gabriela Oprea, MD, Tanvi Dhere, MD. P3145 - Hidden Until the Fall: Traumatic Trigger of Meckel’s Bleed, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.