Naveen Polavarapu, MRCP, CCT1, Geethika Sai Satyavasukiaparna Garaga, MBBS, MRCP2, Somasekhar Rao Kudaravalli, MD, DM1, N. Eshwar Chandra, MD, DNB, FRCR1, P. Siva Charan Reddy, MS, Mch1, G.R. Mallikarjuna, MS, Mch1 1Yashoda hospitals, Hyderabad, Hyderabad, Telangana, India; 2Yashoda hospitals, Hyderabad, Telangana, India Introduction: Gastrointestinal lipomas are unusual, slow growing benign tumors, with gastric lipomas being rarer accounting for only 1% of all gastric tumors and 5% of gastro-intestinal lipomas. 95% of the gastric lipomas are submucosal with sub-serosal lipomas being extremely rare. Usually asymptomatic. Rarely they can cause symptoms like gastric outlet obstruction, GI bleeding, intussusception owing to size and ulceration.
Case Description/
Methods: A 54-year-old-female with no co-morbid conditions, presented to the ED with complaints of sweating, dizziness, associated with melena and hematemesis. Past medical/ surgical/ drug history was insignificant. Physical examination was unremarkable except for pallor. Her hemoglobin was 6.8 gm/dl (baseline 11 g/dl), platelet count 2 lakhs/cu mm, leucocyte count 10,000 cells/cu mm. Rest of the comprehensive metabolic panel was normal. ECG, chest X-Ray, Echocardiogram, ultrasound abdomen was normal. Troponin-I was negative. After initial stabilization in the ED, she was taken up for Upper gastro-intestinal endoscopy which showed a 5-6cm smooth, rounded lesion in the body of the stomach with surface ulcer, with no active ooze, showing positive pillow-sign and tenting-sign. Computerized tomography (CT) scan of the abdomen was done which showed a large, well-defined sub-mucosal mass measuring approximately 55x40 mm, arising from mid-body of the stomach with faint internal inhomogeneity and attenuation between -70 and -80 Hounsfield units (HU) - suggesting gastric lipoma. The patient underwent diagnostic laparoscopy and excision of the sub-mucosal lipoma. Histopathology from the resected specimen showed mature adipocytes, separated by fibrous septa with focal lymphocyte aggregates confirming lipoma. At follow-up, the hemoglobin was stable at 10.8 gm/dl and the patient did not report any further episodes of GI bleed. Discussion: Although rare, gastric lipomas can cause significant life-threatening GI bleed which would warrant intervention. The best diagnostic modalities for gastric lipoma are Endoscopy, Computerized tomography and Endoscopic ultrasound (EUS). The choice of treatment for gastric lipoma remains controversial. A detailed pre-operative evaluation is needed as coincidental separate malignant lesions have been reported by Yamamoto et al in 2004. In our case, as she was symptomatic with GI bleed, she had diagnostic laparoscopy and excision of the sub-mucosal gastric lipoma with positive outcome at follow-up.
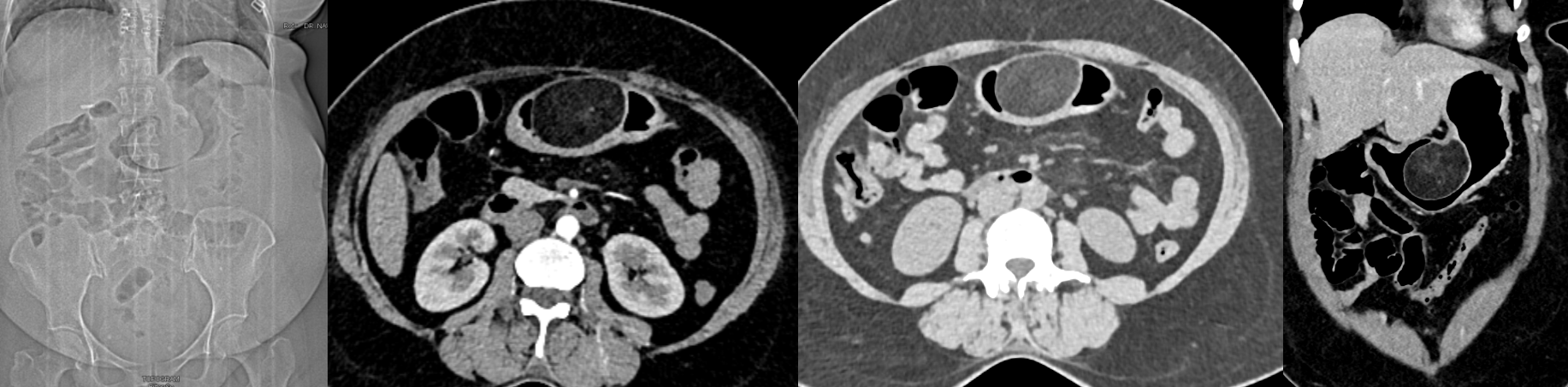
Figure: Computerized tomography images of the abdomen (from left to right: Topogram, axial non-contrast, axial post contrast and post contrast coronal sections) showing a large, well-defined, smoothly marginated homogenous polypoid fast density lesion arising from the lesser curvature of the mid-body of stomach projecting into the lumen - suggestive of Lipoma.
Figure: Figures 1and 2 - Endoscopy images showing smooth, rounded lesion with surface ulcer in the body of the stomach. Figures 3 and 4 - Resected specimen showing well circumscribed lesion with thin fibrous capsule and yellowish cross-section - suggestive of lipoma. Figure 5 - Histopathology image showing capsulated, benign mature appearing adipocytes consistent with lipoma.
Disclosures: Naveen Polavarapu indicated no relevant financial relationships. Geethika Sai Satyavasukiaparna Garaga indicated no relevant financial relationships. Somasekhar Rao Kudaravalli indicated no relevant financial relationships. N. Eshwar Chandra indicated no relevant financial relationships. P. Siva Charan Reddy indicated no relevant financial relationships. G.R. Mallikarjuna indicated no relevant financial relationships.
Naveen Polavarapu, MRCP, CCT1, Geethika Sai Satyavasukiaparna Garaga, MBBS, MRCP2, Somasekhar Rao Kudaravalli, MD, DM1, N. Eshwar Chandra, MD, DNB, FRCR1, P. Siva Charan Reddy, MS, Mch1, G.R. Mallikarjuna, MS, Mch1. P3139 - Gastric Lipoma: A Rare Cause of Gastrointestinal Bleed, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")