University of Iowa Hospitals & Clinics Iowa City, IA
Alp S. Kahveci, MD1, Katelin Durham, MD1, Divya Ashat, MBBS1, Swathi Rajagopal, MD2, Andrew M. Bellizzi, MD1 1University of Iowa Hospitals & Clinics, Iowa City, IA; 2University of Iowa Hospitals and Clinics, Iowa City, IA Introduction: Vitamin deficiencies are common in patients with inflammatory bowel disease (IBD). Guidelines recommend routine screening for vitamin B12 and vitamin D deficiencies, however detection of vitamin E deficiency is uncommon. Here, we present a case of vitamin E deficiency which was diagnosed incidentally on review of histopathology.
Case Description/
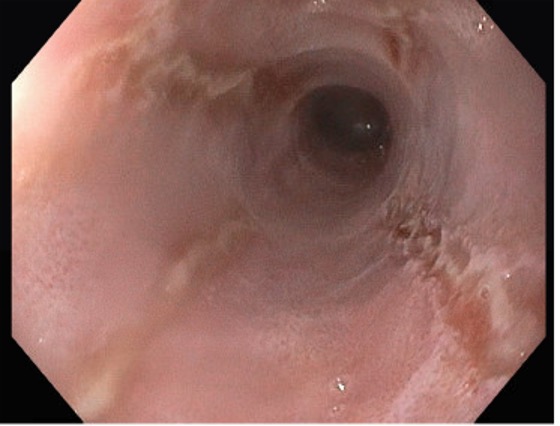
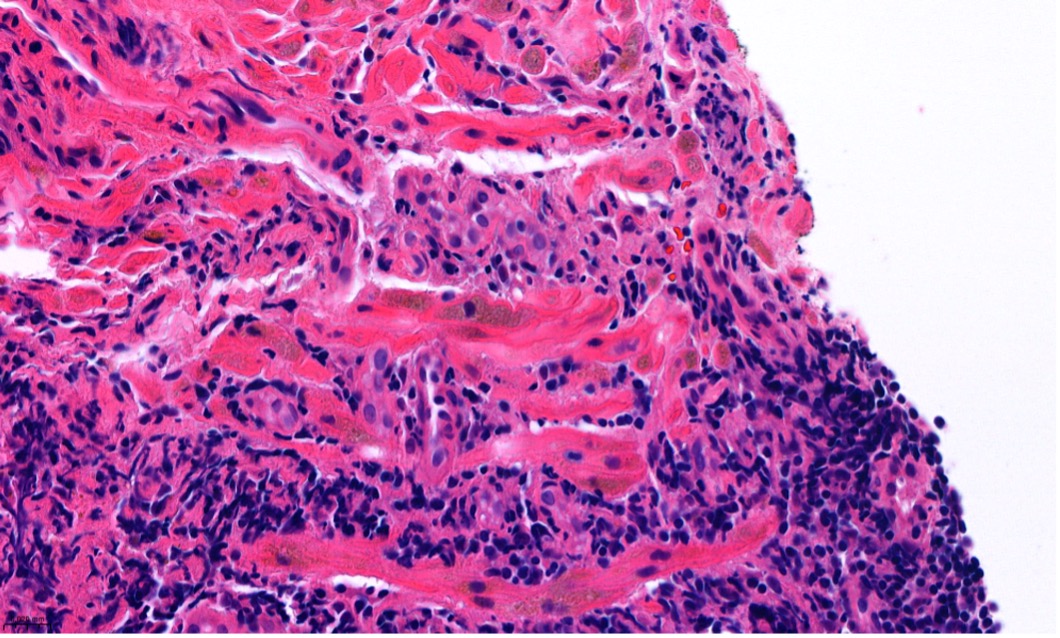
Methods: A 47-year-old female with a history of stricturing ileo-colonic Crohn's disease, status post ileocecal resection, in deep remission with ustekinumab, presented to clinic with new onset dysphagia to solids and odynophagia. She had a 30-pound unintentional weight loss over the past year. Upper endoscopy revealed longitudinal, linear superficial ulcers in the esophagus (Figure 1). Biopsies confirmed herpes simplex virus (HSV) esophagitis. Additionally, golden-brown granular pigment deposits were identified within smooth muscle fibers, consistent with lipofuscin deposition, a histologic finding known as smooth muscle ceroidosis (Figures 2 and 3). Prompted by these findings, serum vitamin E levels were measured and were profoundly low at 0.7 mg/L (reference range 5.5-17.0 mg/L). She was treated with anti-viral therapy for HSV, and vitamin E supplementation (800 IU daily), resulting in resolution of symptoms. Discussion: Vitamin E plays a crucial role in protecting mitochondria from lipid peroxidation. In malabsorptive states, its deficiency can lead to lipofuscin accumulation, a byproduct of lipid peroxidation, within the smooth muscle fibers of the gastrointestinal tract. These granules appear golden brown on H&E staining, leading to the term smooth muscle ceroidosis or brown bowel syndrome. Clinically, patients with vitamin E deficiency may be asymptomatic or may present with subtle neurologic symptoms. Fewer than 70 cases of smooth muscle ceroidosis have been described and have rarely been associated with the development of bowel dilation and pseudo-obstruction. Identification of this finding on esophageal biopsies, as in our case, is exceptionally uncommon. Importantly, its detection led to timely diagnosis and treatment of hypovitaminosis E, potentially preventing more severe complications. We report this case to raise awareness of vitamin E deficiency as a rare but important complication in patients with IBD, and to highlight the utility of histopathologic findings in guiding diagnosis.
Disclosure: This project was sponsored by the Bruce L. Miller & M. Joyce Miller Memorial & Visiting Professorship
Figure: Figure 1: Upper endoscopy. Endoscopic visualization of the esophagus showed linear ulcers suggestive of HSV esophagitis.
Figure: Figure 2: Hematoxylin and eosin stain. Lipofuscin aggregates in the muscularis mucosae of the esophagus, consistent with brown bowel syndrome
Disclosures: Alp Kahveci indicated no relevant financial relationships. Katelin Durham indicated no relevant financial relationships. Divya Ashat indicated no relevant financial relationships. Swathi Rajagopal indicated no relevant financial relationships. Andrew Bellizzi: AstraZeneca (Any division) – Prepared a lecture on low/pan HER2.
Alp S. Kahveci, MD1, Katelin Durham, MD1, Divya Ashat, MBBS1, Swathi Rajagopal, MD2, Andrew M. Bellizzi, MD1. P3367 - A Rare Histopathologic Clue to Vitamin E Deficiency in a Patient With Crohn’s Disease, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.