Ali Shaat, MD1, Ishan Antony, MD2, Akshay Kapoor, MD1, Anand Narasimhan, MD1 1Lahey Hospital and Medical Center, Burlington, MA; 2Beth Israel Lahey Health, Burlington, MA Introduction: Laparoscopic adjustable gastric banding (LAGB) previously emerged as a popular surgical option for managing morbid obesity; however, it has fallen out of favor due to more advanced medical and surgical weight loss options. Despite its decreased utilization, complications arising from the surgery remain clinically significant and often require prompt management. This case highlights advanced endoscopic techniques used to effectively retrieve an eroded gastric band, highlighting their utility as a surgery-sparing intervention.
Case Description/
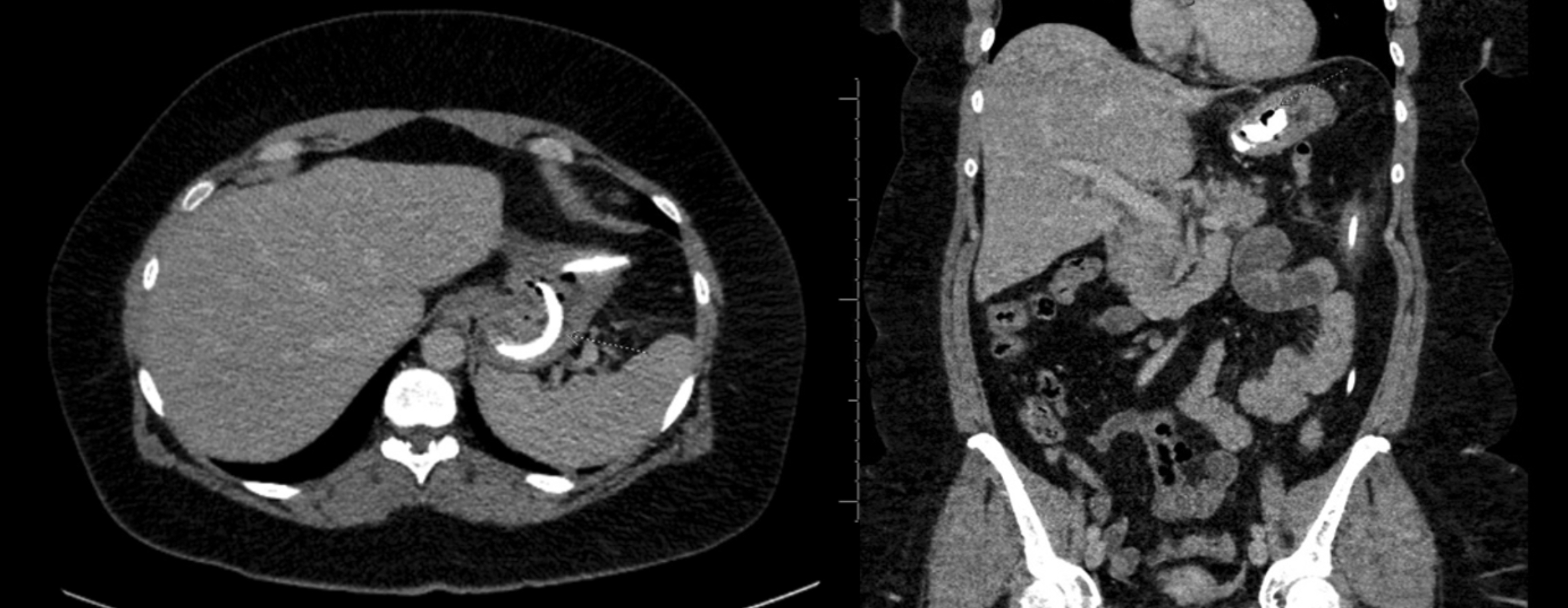
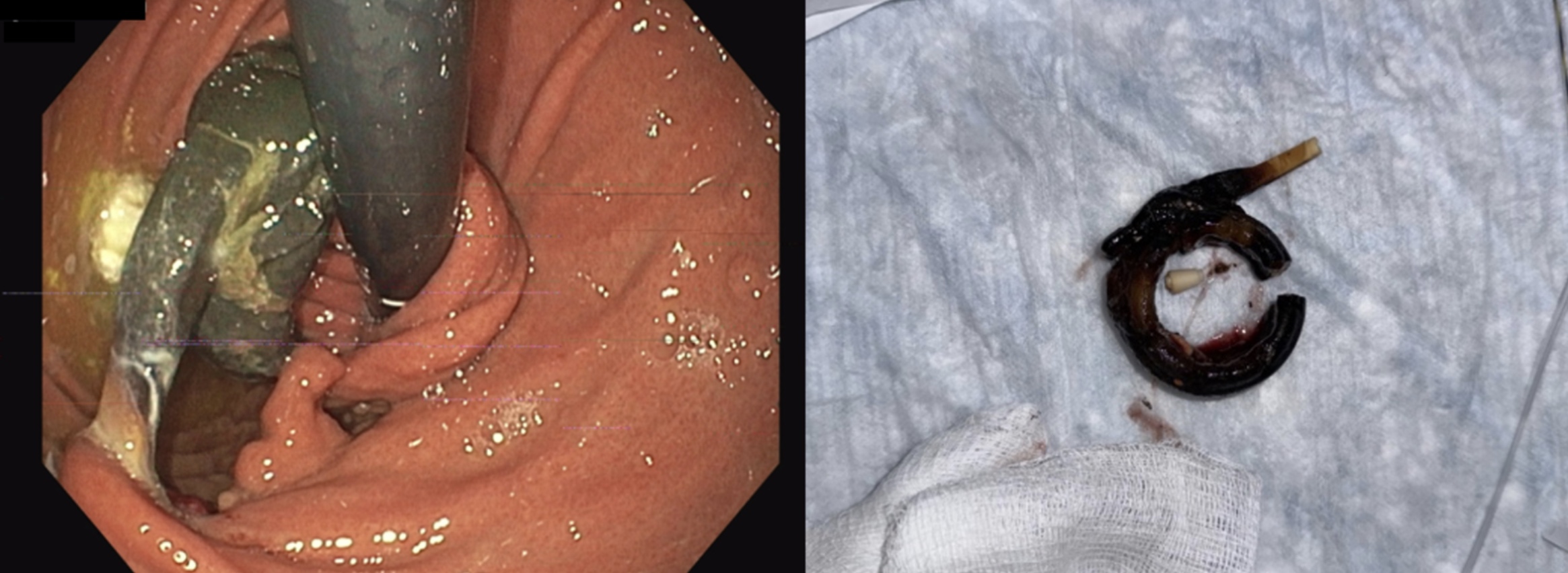
Methods: A 46-year-old female with a history of morbid obesity managed by LAGB 12 years prior, recent initiation of tirzepatide injections, and a prior laparoscopic cholecystectomy presented to the emergency department with severe epigastric pain, nausea, and laboratory findings consistent with acute pancreatitis. Computed tomography (CT) of the abdomen and pelvis demonstrated acute interstitial pancreatitis without biliary ductal dilation, alongside incidental findings of gastric band erosion into the stomach lumen with associated focal fat stranding of the intra-abdominal connecting tubing (Figure 1). Magnetic resonance cholangiopancreatography imaging ruled out a biliary phenomenon and further elucidated these incidental findings. The patient underwent an esophagogastroduodenoscopy, which confirmed complete erosion of the gastric band at the cardia (Figure 2). Endoscopic retrieval was performed by looping a 0.035-inch, 450-cm guidewire around the gastric band and intra-gastric connecting tube, followed by mechanical lithotripsy to sever both components (Figure 2). The gastric band was subsequently removed via endoscopic snare, resulting in minimal mucosal disruption. Post-procedure, the patient reported minimal discomfort, quickly progressed from a liquid to a soft diet, and was discharged the following day. Follow-up CT imaging confirmed successful removal of the gastric band. The residual connecting tubing and subcutaneous port were later removed through a minor outpatient procedure performed by the bariatric surgery team. Discussion: Endoscopic retrieval of eroded gastric bands is a minimally invasive, safe, and effective alternative to surgery. Utilizing aforementioned techniques significantly reduces patient morbidity, hospital stay, and recovery duration. This case underscores the effectiveness of advanced endoscopic techniques as primary management strategies, advocating their broader adoption to decrease dependence on invasive surgical options.
Figure: CT abdomen and pelvis demonstrating gastric band erosion into the stomach lumen, with associated focal fat stranding of the intra-abdominal connecting tube.
Figure: (Left) Endoscopic view of the fully eroded gastric band at the cardia. (Right) Retrieved gastric band following endoscopic transection at the band junction and intragastric connecting tube.
Disclosures: Ali Shaat indicated no relevant financial relationships. Ishan Antony indicated no relevant financial relationships. Akshay Kapoor indicated no relevant financial relationships. Anand Narasimhan indicated no relevant financial relationships.
Ali Shaat, MD1, Ishan Antony, MD2, Akshay Kapoor, MD1, Anand Narasimhan, MD1. P3587 - Endoscopic Retrieval of an Eroded Gastric Band: A Minimally Invasive Alternative to Surgical Intervention, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.