University of Arizona College of Medicine - Phoenix Phoenix, AZ
Award: ACG Presidential Poster Award
Pradhan Hariharan, BS1, Vanessa Eller, MD2, Joseph Solomon, BS1, Kevin Liu, MD3 1University of Arizona College of Medicine - Phoenix, Phoenix, AZ; 2University of Arizona College of Medicine, Phoenix, Phoenix, AZ; 3Banner University Medical Center, Phoenix, AZ Introduction: In patients with Roux-en-Y gastric bypass (RYGB), marginal ulceration at the gastrojejunal anastomosis is a complication that can lead to perforation requiring emergency surgery. Recently, endoscopic techniques have emerged as potential minimally invasive alternatives to surgical repair for managing complications related to refractory marginal ulcers. X-Tack is a novel through-the-scope helical tack and suture system that can be used for endoscopic closure of intraluminal defects. We report a case of combined endoscopic therapy with X-Tack and enteral stent placement with successful non-operative healing of a perforated gastrojejunal ulcer.
Case Description/
Methods: A 58-year-old male with a history of RYGB one year ago was transferred emergently to our institution after presenting to an outside hospital with severe abdominal pain with imaging demonstrating intraperitoneal free air. Given concern for perforated ulcer, he underwent emergent exploratory laparoscopy and was found to have purulent peritonitis with multiple abscess pockets, dense adhesions surrounding the gastrojejunal anastomosis, and complete dehiscence of the gastrojejunal anastomosis. An EGD was performed which visualized a deep cratered circumferential ulcer measuring 5 cm in length on the anterior side of the anastomosis with evidence of dehiscence at the anastomotic site. Combined endoscopic therapy was performed with closure of the dehiscence with the X-Tack suturing device followed by enteral stent placement across the gastrojejunal anastomosis. First, a series of 8 tacks were deployed in a figure 8 pattern to approximate the dehiscence. This was technically challenging given significant submucosal fibrosis around the ulcer bed. After suture deployment, there was still concern for small amount of leakage of contrast on fluoroscopic views. An 18 mm x 14 cm through-the-scope covered metal stent was then placed across the gastrojejunal anastomosis and endoscopic suture fixation with subsequent injection of contrast confirming no extravasation. A follow-up EGD 8 weeks later revealed complete resolution of the dehiscence with a small ulcer remaining at the site without any residual leak. Discussion: This case illustrates the role of combined endoscopic therapy with endoscopic suturing and stent placement for non-operative treatment of a perforated marginal ulcer. Future studies are needed to better understand long-term outcomes of the X-Tack closure system and when monotherapy vs. combined endoscopic therapy should be considered.
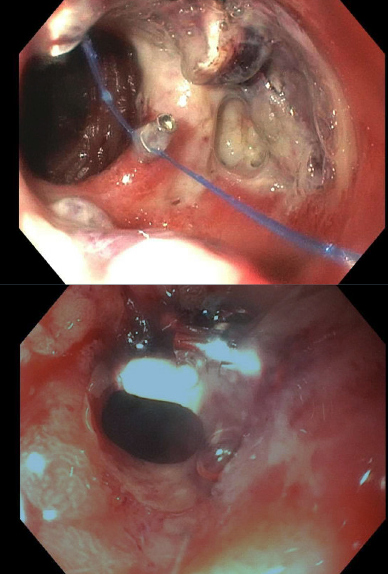
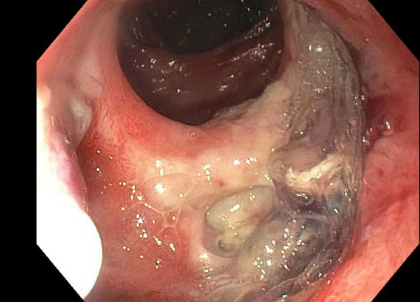
Figure: Large Gastrojejunal Hemicircumferential Anastomotic Ulcer with Open Dehiscence
Figure: X-Tack Deployment To Appose the Ulcer and Area of Dehiscence
Disclosures: Pradhan Hariharan indicated no relevant financial relationships. Vanessa Eller indicated no relevant financial relationships. Joseph Solomon indicated no relevant financial relationships. Kevin Liu indicated no relevant financial relationships.
Pradhan Hariharan, BS1, Vanessa Eller, MD2, Joseph Solomon, BS1, Kevin Liu, MD3. P3580 - Endoscopic Closure of Post-RYGB Perforation Using X-Tack System, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")