Washington State University Elson S. Floyd School of Medicine Auburn, WA
Harneet Sangha, BS1, Nuria Perez-Reyes, MD2, Mohit Girotra, MD3 1Washington State University Elson S. Floyd School of Medicine, Spokane, WA; 2CellNetix Pathology and Laboratories, Seattle, WA; 3Swedish First Hill Medical, Seattle, WA Introduction: Endoscopic ultrasonography (EUS) with fine needle aspiration (FNB) plays a central role in the characterization of gastrointestinal (GI) tract subepithelial lesions. While gastrointestinal stromal tumors (GIST) represent a frequent suspicion when a hypoechoic intramural lesion is encountered, it is feasible that benign non-GI pathology should yield the same features.
We report here an extremely uncommon case of a benign ovary embedded entirely in the rectosigmoid colon wall on EUS-FNB in a patient who had previously undergone hysterectomy.
Case Description/
Methods: A 42-year-old woman with a history of hysterectomy for uterine fibroids presented with diarrhea, bloating, and intermittent hematochezia. CT abdomen/pelvis revealed thickened bowel loops, prompting a colonoscopy. A 2.4 × 1.8 cm bulging lesion in the rectosigmoid colon was noted, without intraluminal mass. EUS showed a heterogeneously hypoechoic lesion seemingly in the fourth colonic wall layer (muscularis propria), but overall findings were not convincing for GIST, due to involvement of other layers as well. EUS-guided FNB was performed using a 22G needle with three passes, and tattoo was placed for surgical localization.
On-site cytology initially suspected spindle cell neoplasm. However, final histopathology revealed benign ovarian stroma and corpus luteum–like cells. Immunohistochemical staining was positive for Progesterone receptor, WT1, inhibin, and CD56, confirming ovarian origin. Notably, the patient had retained ovaries despite prior hysterectomy. Pelvic ultrasound revealed a normal right ovary and a left ovary with a dominant follicle and corpus luteum–like structure, embedded in colon wall.
Considering the lesion's involvement of colon wall and symptoms of the patient, robotic left oophorectomy was done. Intraoperatively, the ovary was found to be heavily adherent and embedded to the rectosigmoid colon, necessitating extensive adhesiolysis and serosal repair. Discussion: This is a rare presentation of ovarian tissue mimicking GIST in the colon wall. Retained ovaries following hysterectomy are not uncommon, but translocation or dense bands resulting in transmural embedding is extremely uncommon. It highlights the importance of histopathologic evidence before deciding management options. EUS-FNB and immunohistochemistry were instrumental in establishing the diagnosis and in planning appropriate surgical management.
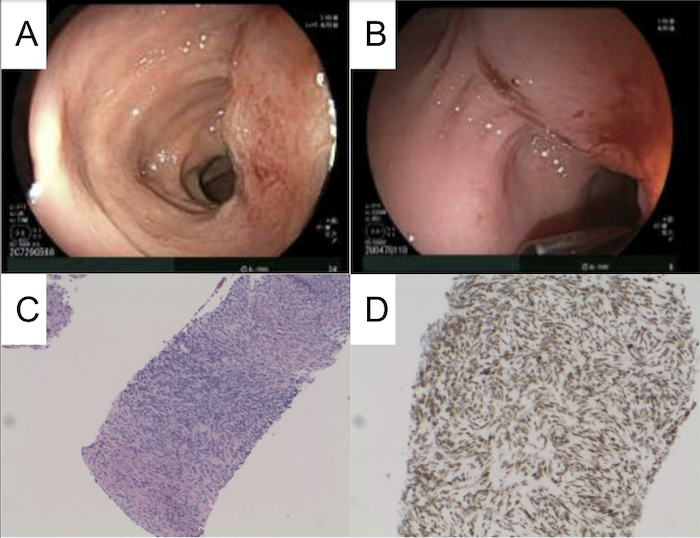
Figure: A/B: Colonoscopy images with recto-sigmoid colon wall intra-mural mass, with inflammatory appearance; C: Ovarian stroma with characteristic spindle cells and prominent vasculature; D: WT1 immunohistochemical stain highlighting nuclear positivity in ovarian stromal cells
Disclosures: Harneet Sangha indicated no relevant financial relationships. Nuria Perez-Reyes indicated no relevant financial relationships. Mohit Girotra indicated no relevant financial relationships.
Harneet Sangha, BS1, Nuria Perez-Reyes, MD2, Mohit Girotra, MD3. P3577 - Ovary Embedded Within the Colon Wall: An Unusual Case of Colon Wall Mass Diagnosed With Endoscopic Ultrasound-Guided Fine Needle Biopsy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")