P6043 - Recurrent Pancreatitis in a Patient With Familial Partial Lipodystrophy Complicated by Mesenteric Thromboses, Non-Cirrhotic Portal Hypertension and Chylous Ascites
Division of Gastroenterology and Hepatology, Center for Digestive Health, Virginia Mason Franciscan Health Seattle, WA
Award: ACG Presidential Poster Award
Muaaz Masood, MD1, Amita Kasar, MD2, Erin Forsythe, DNP, ARNP3, Wendy Hsu, MD3, Vikram Anand, MD3 1Division of Gastroenterology and Hepatology, Center for Digestive Health, Virginia Mason Franciscan Health, Seattle, WA; 2Poplar Bluff Regional Medical center, Poplar Bluff, MO; 3Virginia Mason Franciscan Health, Seattle, WA Introduction: Chylous ascites is a rare complication of pancreatitis and involves accumulation of triglyceride-rich lymphatic fluid in the peritoneal cavity. Familial partial lipodystrophy (FPLD) is a genetic predisposition to abnormal distribution of adipose tissue, and can be associated with hypertriglyceridemia, insulin resistance, diabetes and steatotic liver disease. We report a case of recurrent pancreatitis in a patient with FPLD resulting in mesenteric thromboses complicated by non-cirrhotic portal hypertension and chylous ascites.
Case Description/
Methods: A 55-year-old man with type 3c diabetes, FPLD (Dunningan-type), severe hypertriglyceridemia, and coronary artery disease who had several episodes of pancreatitis over the past 20 years. More recently, he presented with cholecystitis, pancreatitis, severe gastric outlet obstruction (GOO) and ascites. He underwent endoscopic ultrasound-guided cholecystoduodenostomy which drained brown/purulent fluid, and an endoscopic ultrasound-guided gastroenterostomy (EUS-GE). Additionally, he was noted to have small esophageal varices, perigastric varices and portal hypertensive gastropathy. A diagnostic paracentesis was consistent with chylous ascites. Diuresis with furosemide and spironolactone was limited by episodes of acute kidney injury and hyponatremia, and he ultimately required serial paracenteses. Due to persistent GOO, a second EUS-GE was performed and the patient was transitioned to total parenteral nutrition. He was also noted to have thrombosis of the main portal and superior mesenteric veins, thereafter requiring anticoagulation. He was not a candidate for TIPS or thrombectomy. Discussion: Our patient’s recurrent pancreatitis was likely due to a combination of biliary sludge and previously severe hypertriglyceridemia (peak triglyceride level 4,273 mg/dL, normal range < 150 mg/dL) requiring medical therapy. He ultimately developed cholecystitis and severe GOO requiring multiple advanced endoscopic treatments. Chylous ascites can occur in pancreatitis due to compression of the lymphatic system, direct damage by pancreatic enzymes and leakage of chyle due to portal vein thrombosis and, with recurrent episodes of pancreatitis, the long-term sequela of non-cirrhotic portal hypertension. Management of chylous ascites includes a high-protein, low-fat diet with medium-chain triglycerides and somatostatin analogues. Treatment of metabolic complications is the mainstay for FPLD.
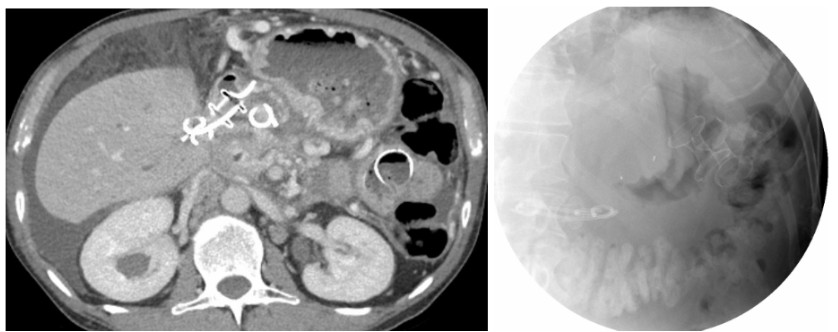
Figure: Panel A. Axial (left) computed tomography scan of the abdomen and pelvis with intravenous contrast revealed a distended stomach, endoscopic ultrasound-guided cholecystoduodenostomy with two double pigtail stents through the stent, and two endoscopic ultrasound-guided gastroenterostomies in place. The fluoroscopic image (right) also demonstrated the endoscopic ultrasound-guided cholecystoduodenostomy with two double pigtail stents through the stent, and two endoscopic ultrasound-guided gastroenterostomies in place.
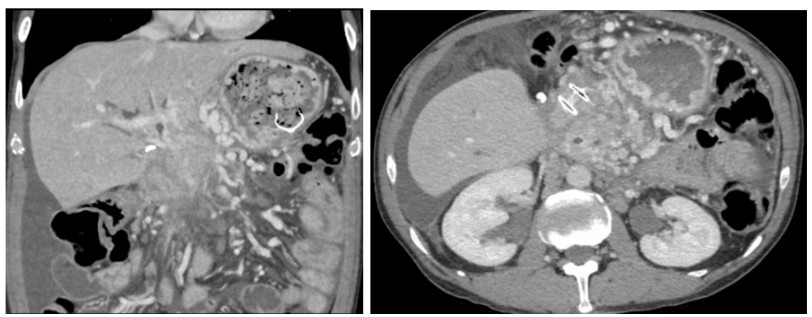
Figure: Panel B. Coronal (left) and axial (right) computed tomography scan of the abdomen and pelvis with intravenous contrast revealed chronic occlusion of the main portal vein, superior mesenteric vein, and splenic vein with extensive collaterals, distended stomach, perihepatic ascites, an endoscopic ultrasound-guided cholecystoduodenostomy and an endoscopic ultrasound-guided gastroenterostomy in place.
Disclosures: Muaaz Masood indicated no relevant financial relationships. Amita Kasar indicated no relevant financial relationships. Erin Forsythe indicated no relevant financial relationships. Wendy Hsu indicated no relevant financial relationships. Vikram Anand indicated no relevant financial relationships.
Muaaz Masood, MD1, Amita Kasar, MD2, Erin Forsythe, DNP, ARNP3, Wendy Hsu, MD3, Vikram Anand, MD3. P6043 - Recurrent Pancreatitis in a Patient With Familial Partial Lipodystrophy Complicated by Mesenteric Thromboses, Non-Cirrhotic Portal Hypertension and Chylous Ascites, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


.jpg "Muaaz Masood, MD photo")