Icahn School of Medicine at Mount Sinai Jamaica, NY
Ahmed Elhawary, MD1, Mohamed Eldesouki, MD2, Joseph Odin, MD3 1Icahn School of Medicine at Mount Sinai, Jamaica, NY; 2Saint Michael's Medical Center, New York Medical College, Newark, NJ; 3Icahn School of Medicine at Mount Sinai, Manhattan, NY Introduction: Khat is a plant cultivated and consumed primarily in the Arabian and East African countries. Chewing khat has been a longstanding social tradition in these regions since the 13th century. In the US, Khat is classified as a controlled substance, making its possession or use illegal. As a result, patients may be reluctant to disclose their khat use to their physicians.
Case Description/
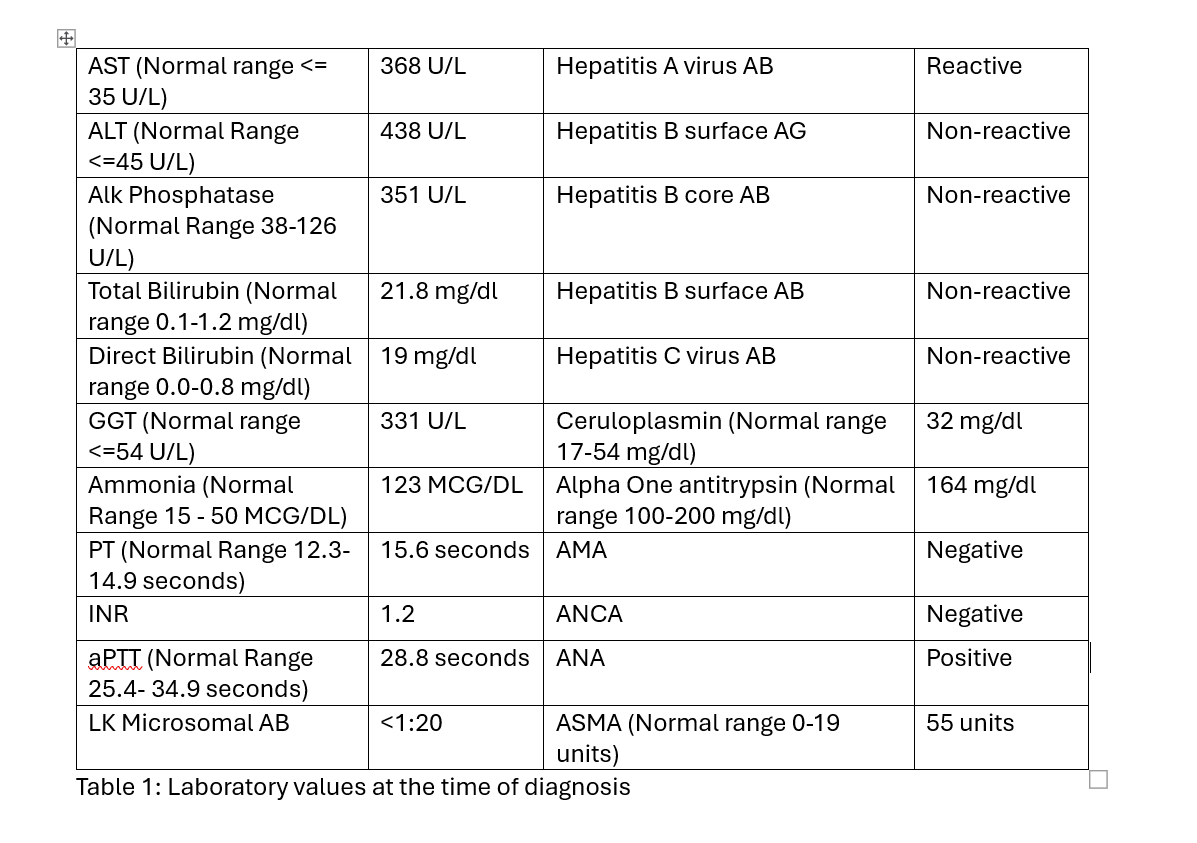
Methods: A 25-year-old male patient, who immigrated recently from Yemen, with a past medical history of hepatitis and possible cirrhosis, presented with worsening jaundice and dark urine. Physical examination showed normal vital signs but there were scleral icterus and jaundiced skin without any abdominal tenderness. Initial labs showed AST 368, ALT 438, Alkaline Phosphatase 351, total bilirubin 21.8, direct bilirubin 19, GGT 331, ammonia 123, PT 15.6, INR 1.2, aPTT 28.8. The viral hepatitis panel was negative, except for a history of hepatitis A indicated by IgG. Alpha one antitrypsin and ceruloplasmin were normal. ANCA and anti mitochondrial antibodies were negative. MRCP showed liver cirrhosis without any hepatic mass or portal hypertension. Although ANA and anti-smooth muscle antibodies were positive, liver biopsy was consistent with drug-induced hepatotoxicity "marked cholestasis with feathery degeneration and patchy lobular necroinflammation, enlarged portal tract with mild lymphoplasmacytic inflammation mixed with eosinophils, bile duct damage and reaction”. Upon questioning the patient about any drug abuse, he reported using Khat frequently. Six years later the patient was presented with decompensated liver cirrhosis, ascites, and spontaneous bacterial peritonitis. MELD-Na score: 29 and MELD score: 26. EGD showed esophageal varices. MRCP showed liver cirrhosis with no HCC. The patient was listed for liver transplantation during this admission and underwent the LT on 11/2019.
Discussion: The first documented case of acute hepatitis linked to khat use was reported in the UK in 2005. The exact mechanism behind khat-induced liver damage remains unclear. However, there is a theory suggests that liver toxicity is caused by khat alkaloids, which undergo extensive hepatic metabolism. Alternative theories propose that khat use can trigger autoimmune mechanisms, leading to liver injury in individuals with a genetic predisposition. Further research is needed to better understand the underlying mechanisms of khat-induced liver injury, with the goal of developing effective treatment options for this condition.
Figure: Laboratory values at the time of diagnosis
Disclosures: Ahmed Elhawary indicated no relevant financial relationships. Mohamed Eldesouki indicated no relevant financial relationships. Joseph Odin indicated no relevant financial relationships.
Ahmed Elhawary, MD1, Mohamed Eldesouki, MD2, Joseph Odin, MD3. P6118 - Liver Transplantation Due to Khat Ingestion, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")