North Shore University Hospital - Northwell Health Manhasset, NY
Jade Pace, MD1, Ahmed Aboseria, MD2, Ravi Patel, MD1, Syed E. Ahmad, MD1 1North Shore University Hospital - Northwell Health, Manhasset, NY; 2North Shore University Hospital - Northwell Health, Brooklyn, NY Introduction: Idiopathic hepatic granulomas are a diagnostic mystery, yet represent up to 50% of cases, typically non-necrotizing. Necrotizing forms are associated with infections like tuberculosis (TB) or fungi. Moreover, primary presentation as fever of unknown origin (FUO) is exceptionally rare. We present a case of idiopathic granulomatous hepatitis (IGH) with necrotizing granulomas manifesting as recurrent FUO.
Case Description/
Methods: A woman in her early fifties from Uzbekistan with remote hepatitis B presented with over six months of fevers, night sweats, weight loss, and lower extremity edema. Initial evaluation at an outside hospital – Computed Tomography (CT), cardiac Magnetic Resonance Imaging (MRI) and Transthoracic Echocardiogram (TTE) – was non-diagnostic. Hepatology, Rheumatology, and Infectious Disease teams were consulted. Notable diagnostic workup is shown in Table 1.
MRI revealed bilobar, peripherally enhancing hepatic lesions (Figure 1). Surgical liver biopsy showed necrotizing granulomatous inflammation with rare broken hyphal forms, which was determined to be the cause of her recurrent fevers. Despite initial treatment with posaconazole, symptoms worsened. Sarcoidosis and Still's Disease were considered but deemed unlikely due to normal angiotensin-converting enzyme (ACE) levels and inconsistent presentation. Because of ferritin and IL-2 elevation, colchicine was trialed but was complicated by influenza-related fevers. She was discharged on oral 32mg methylprednisolone once daily, trimethoprim/sulfamethoxazole once daily for prophylaxis, and furosemide for hypervolemia. Patient’s defervescence was confirmed during outpatient appointments. Fevers recurred briefly on doses of methylprednisolone below 20mg. Discussion: This case illustrates a rare presentation of biopsy-proven necrotizing hepatic granulomas manifesting as FUO. Despite extensive workup across multiple hospitals and specialties, no clear infectious, autoimmune, or malignant etiology was ascertained. Elevated ferritin and IL-2 levels and positive response to corticosteroids indicated a hyperinflammatory state. The aggregate of this workup confirmed the diagnosis of idiopathic granulomatous hepatitis. IGH remains a diagnosis of exclusion, emphasizing the importance of liver biopsy and interdisciplinary evaluation.
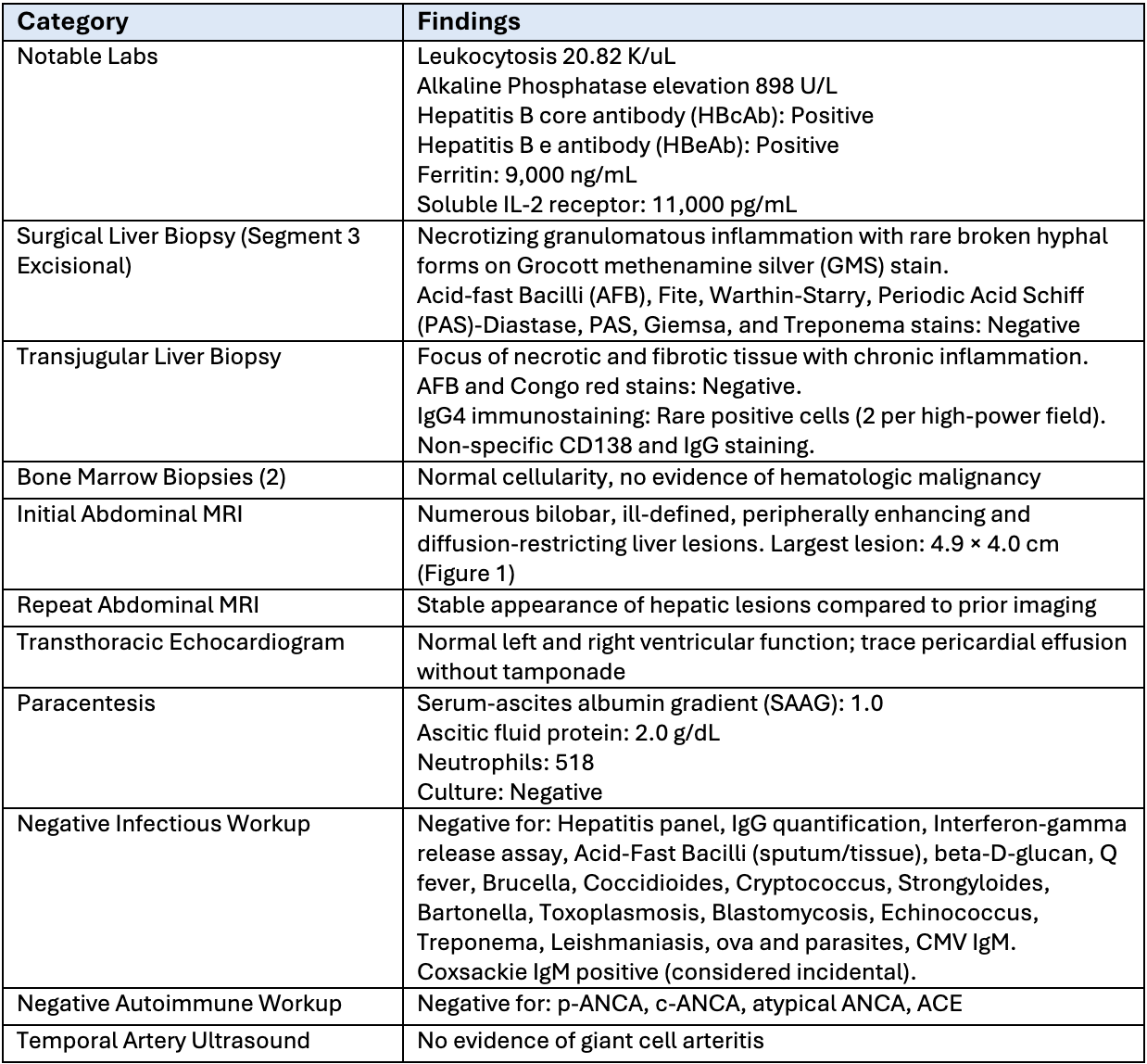
Figure: Table 1. Summary of diagnostic workup.
Figure: Figure 1. MR abdomen demonstrating numerous bilobar ill-defined peripherally enhancing and diffusion restricting liver lesions. Conglomerate lesion at the dome measuring 4.9 x 4 cm viewable in this cut.
Disclosures: Jade Pace indicated no relevant financial relationships. Ahmed Aboseria indicated no relevant financial relationships. Ravi Patel indicated no relevant financial relationships. Syed Ahmad indicated no relevant financial relationships.
Jade Pace, MD1, Ahmed Aboseria, MD2, Ravi Patel, MD1, Syed E. Ahmad, MD1. P6109 - Fever of Unknown Origin Secondary to Necrotizing Hepatic Granulomas: A Rare Case of Idiopathic Granulomatous Hepatitis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")