Staten Island University Hospital Staten Island, NY
Daniel Kalta, DO, MS1, Rajarajeshwari Ramachandran, MD2, Tonya DeVaul, NP3, Heidi Budke, MD3, Vinaya Gaduputi, MD3 1Staten Island University Hospital, Staten Island, NY; 2Fresno Veterans Affairs Medical Center, Fresno, CA; 3Blanchard Valley Health System, Findlay, OH Introduction: We are presenting a case of gastrointestinal involvement of mantle cell lymphoma diagnosed during evaluation of early satiety, bloating, and change in bowel habits.
Case Description/
Methods: A 75-year-old male with end-stage-renal-disease on hemodialysis, and chronic anemia, presented to the gastroenterology clinic for evaluation of early satiety, bloating, new onset change in stool caliber and constipation. He denied dysphagia, nausea, vomiting, abdominal pain, fevers, chills, night sweats, melena, hematochezia or unintentional weight loss. On examination, the abdomen was soft, non-tender, without organomegaly or ascites.
Laboratory data: white cell count 11,200/microliter (72.7% neutrophils, 20.1% lymphocytes, 4.8% monocytes, 1.6% eosinophils, and 0.6% basophils), hemoglobin 7.3 g/dL, platelet count 155,000/microliter, sodium 138 mEq/L, potassium 4.3 mEq/L, chloride 103 mEq/L, creatinine 8.14 mg/dL, alanine aminotransferase (ALT) 15 U/L, aspartate aminotransferase (AST) 15 U/L, alkaline phosphatase 53 U/L, total bilirubin 1.2 mg/dL, total protein 5.9 g/dL, albumin 3 g/dL.
Given the history of early satiety, bloating, and new change in bowel habits, bidirectional endoscopy was recommended, and the patient agreed.
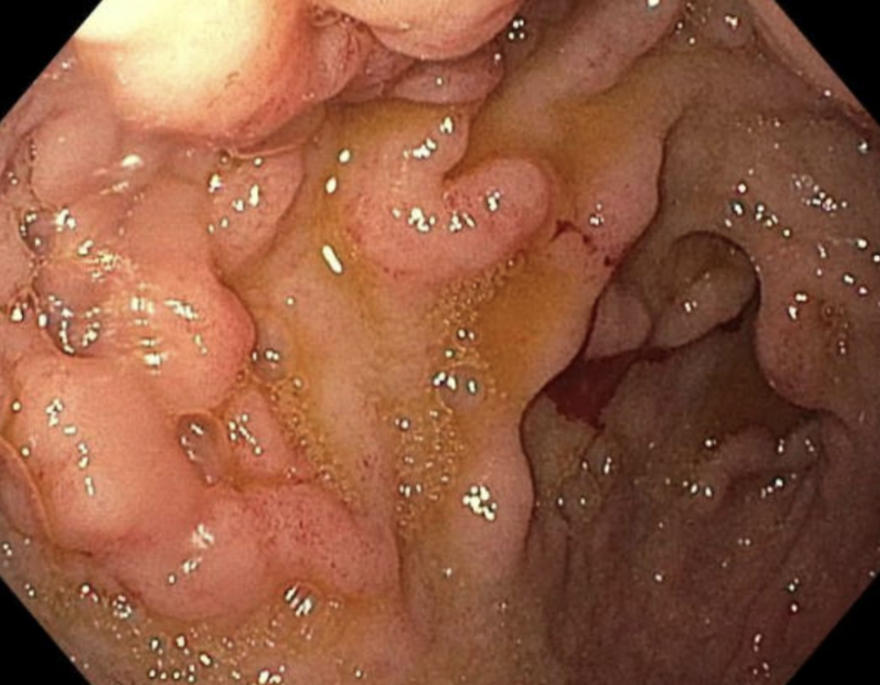
Esophagogastroduodenoscopy (EGD): Normal esophagus. Gastric folds were thick and with mild antral erythema. There were inflamed, prominent mucosal folds in the duodenal bulb (image 1) and second portion of the duodenum was normal. No gastric or duodenal mass lesions. Biopsies from the stomach and the prominent folds in the duodenal bulb demonstrated scattered clusters of plasma cells and few lymphocytes (composed of small lymphocytes) in the prominent lymphoid aggregates. Immnostains of the lymphocytes were positive for CD20, CD5, and with nuclear staining of cyclin D1. Overall, the findings were consistent with mantle cell lymphoma (MCL).
Colonoscopy: Good bowel preparation. 3 mm sessile transverse colon polyp removed with cold forceps. No colitis or colonic masses seen. Microscopic examination of the colon polyp was positive for findings consistent with MCL.
Following the identification of MCL, the oncology team was consulted for further management. PET scan ruled out nodal involvement. Bone marrow biopsy demonstrated 10-20% involvement with MCL. Discussion: After multidisciplinary evaluation, our patient was diagnosed with indolent MCL, which carries a favorable diagnosis. He is currently being observed by the oncology team.
Figure: Image 1: EGD image of prominent mucosal folds in the duodenal bulb
Disclosures: Daniel Kalta indicated no relevant financial relationships. Rajarajeshwari Ramachandran indicated no relevant financial relationships. Tonya DeVaul indicated no relevant financial relationships. Heidi Budke indicated no relevant financial relationships. Vinaya Gaduputi indicated no relevant financial relationships.
Daniel Kalta, DO, MS1, Rajarajeshwari Ramachandran, MD2, Tonya DeVaul, NP3, Heidi Budke, MD3, Vinaya Gaduputi, MD3. P6263 - Unraveling a Hidden Culprit: A Case of Gastrointestinal Involvement of Mantle Cell Lymphoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Daniel Kalta, DO, MS photo")