P6261 - Regression of Duodenal Adenomatous Polyposis in Response to Combination FOLFOX/Nivolumab for the Treatment of Gastric Adenocarcinoma in a Patient With Familial Adenomatous Polyposis Syndrome
Malak Munir, MD, Srinivas Gaddam, MD, MPH, Barham K. Abu Dayyeh, MD, MPH, Simon K.. Lo, MD, FACG Cedars-Sinai Medical Center, Los Angeles, CA Introduction: Duodenal adenomas (DA) in Familial Adenomatous Polyposis (FAP) patients carry a lifetime cancer risk of 2%-18% . Current management involves endoscopic surveillance with Spiegelman staging and selective polypectomy. Studies have failed to identify effective preventative treatments, with scarce evidence supporting underlying mechanisms governing their development. The unique immunological microenvironment of the duodenum may hold key insights into pathogenesis and potential therapeutic targets, however immune mechanisms are largely unexplored as therapeutic targets despite emerging immunomodulatory treatments. We present a case of DA regression in an FAP patient receiving FOLFOX-nivolumab combination therapy for metastatic gastric adenocarcinoma.
Case Description/
Methods: A 43-year-old woman with Hashimoto thyroiditis and FAP underwent annual surveillance since 2009. History includes colectomy with ileoanal J-pouch reconstruction and ampullectomy for large ampullary adenoma. Endoscopy revealed high burden fundal gland polyps (10-50mm) and extensive DA (5-25mm) with low burden jejunal polyps. During 2024 surveillance, gastric ulcer biopsy confirmed moderate to poorly differentiated adenocarcinoma. Testing showed intact expression of mismatch repair proteins, PD-L1 positive, with metastases to liver and lymph nodes on PET-CT. She received FOLFOX-nivolumab for 8 cycles then 5-FU-nivolumab maintenance, she has currently achieved stable disease. After 27 cycles, endoscopy showed complete gastric ulcer resolution and remarkable DA improvement (size ≤5mm). Discussion: We observed significant DA improvement following FOLFOX-nivolumab therapy. Whether regression is attributable to FOLFOX, nivolumab, or synergistic interaction remains unclear. We identified only two case reports documenting DA regression with FOLFOX alone; our patient showed a more dramatic response. Additionally, reported complete colorectal adenoma regression following FOLFOX-durvalumab supports our hypothesis that immunotherapy may enhance adenoma regression. The duodenum possesses rich immunological microenvironment with abundant gut-associated lymphoid tissue, regulatory T-cells, and antigen-presenting cells, creating unique milieu where immunotherapy might exert effects. Nivolumab's PD-1 blockade may mediate local cytotoxic T-cell activity against neoplastic cells. This synergistic hypothesis is compelling given immunosurveillance's hypothesized role in preventing adenoma-to-carcinoma progression.
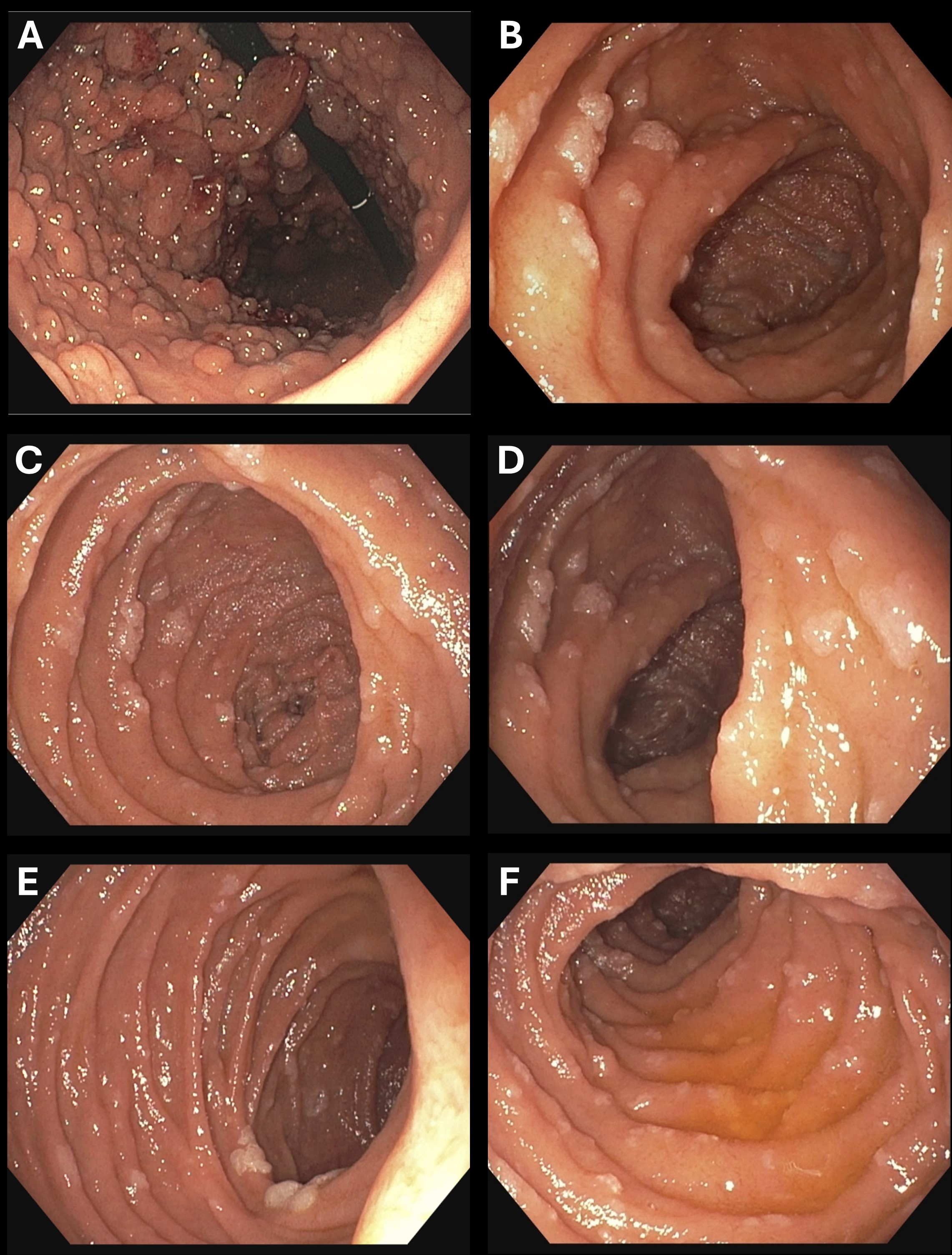
Figure: Figure 1. Endoscopic Images (2024). A: Extension and Size of FGP; B-F Duodenal Adenomas at Cancer Diagnosis.
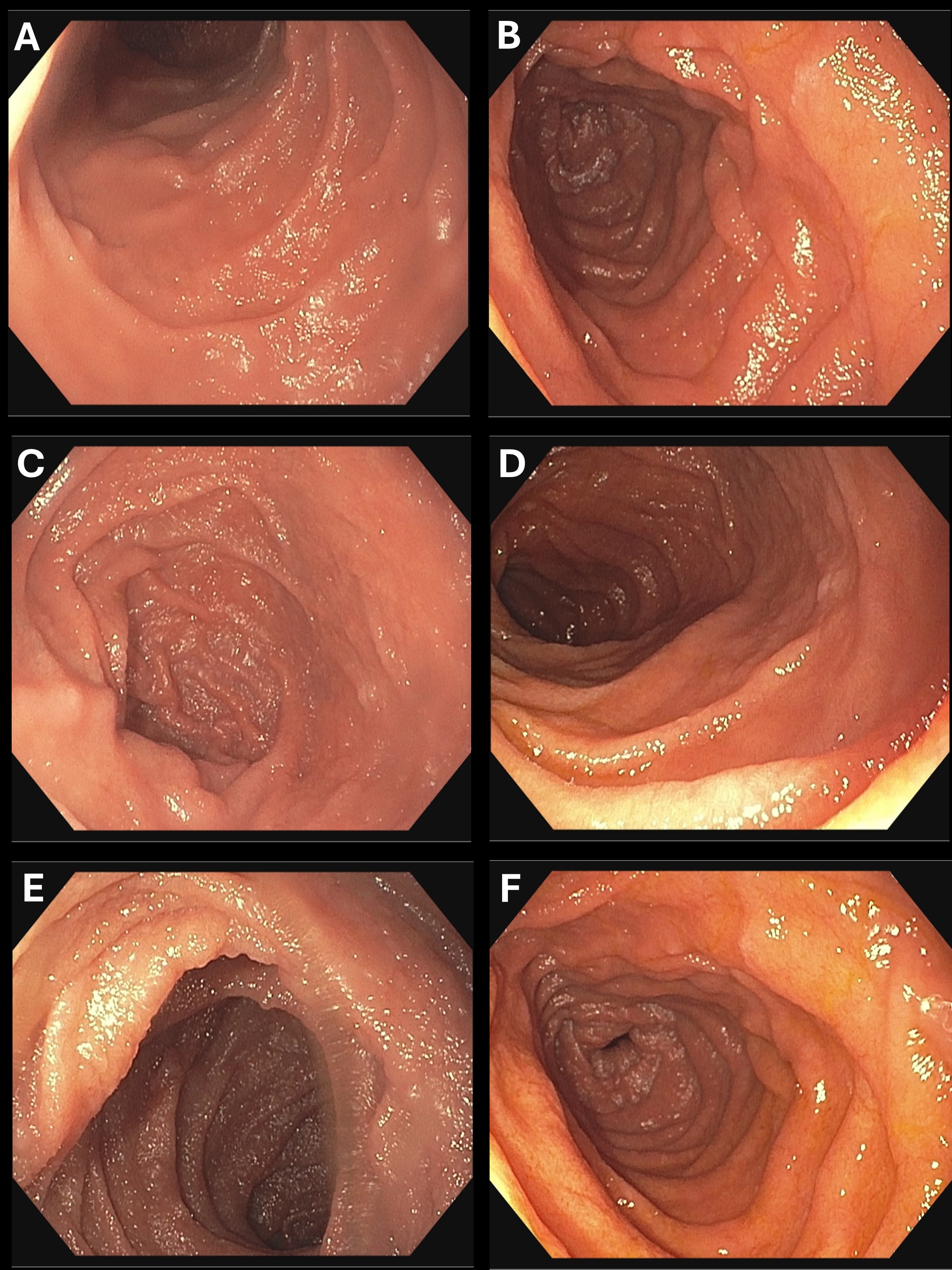
Figure: Figure 2. Endoscopic Images (2025). A-F: Regression of Duodenal Adenomas Post-treatment with combined chemo/immunotherapy
Disclosures: Malak Munir indicated no relevant financial relationships. Srinivas Gaddam indicated no relevant financial relationships. Barham Abu Dayyeh indicated no relevant financial relationships. Simon Lo indicated no relevant financial relationships.
Malak Munir, MD, Srinivas Gaddam, MD, MPH, Barham K. Abu Dayyeh, MD, MPH, Simon K.. Lo, MD, FACG. P6261 - Regression of Duodenal Adenomatous Polyposis in Response to Combination FOLFOX/Nivolumab for the Treatment of Gastric Adenocarcinoma in a Patient With Familial Adenomatous Polyposis Syndrome, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.