University of Virginia School of Medicine Charlottesville, VA
Ana S. Lopez Alvarez, BS, MS1, Claire F. Maher, BA1, Emily Minor, MD, PhD2, Rebecca Haug, MD3 1University of Virginia School of Medicine, Charlottesville, VA; 2University of Virginia, Charlottesville, VA; 3University of Virginia Medical Center, Charlottesville, VA Introduction: Small bowel tumors are rare and difficult to diagnose due to relative inaccessibility and non-specific symptomatology. Capsule endoscopy (CE) is indicated for the identification and localization of small bowel tumors however is typically contraindicated in patients with known or suspected strictures or obstructions to avoid capsule retention. This case highlights a unique approach to tumor localization in a patient with recurrent small bowel obstruction (SBO) using capsule endoscopy.
Case Description/
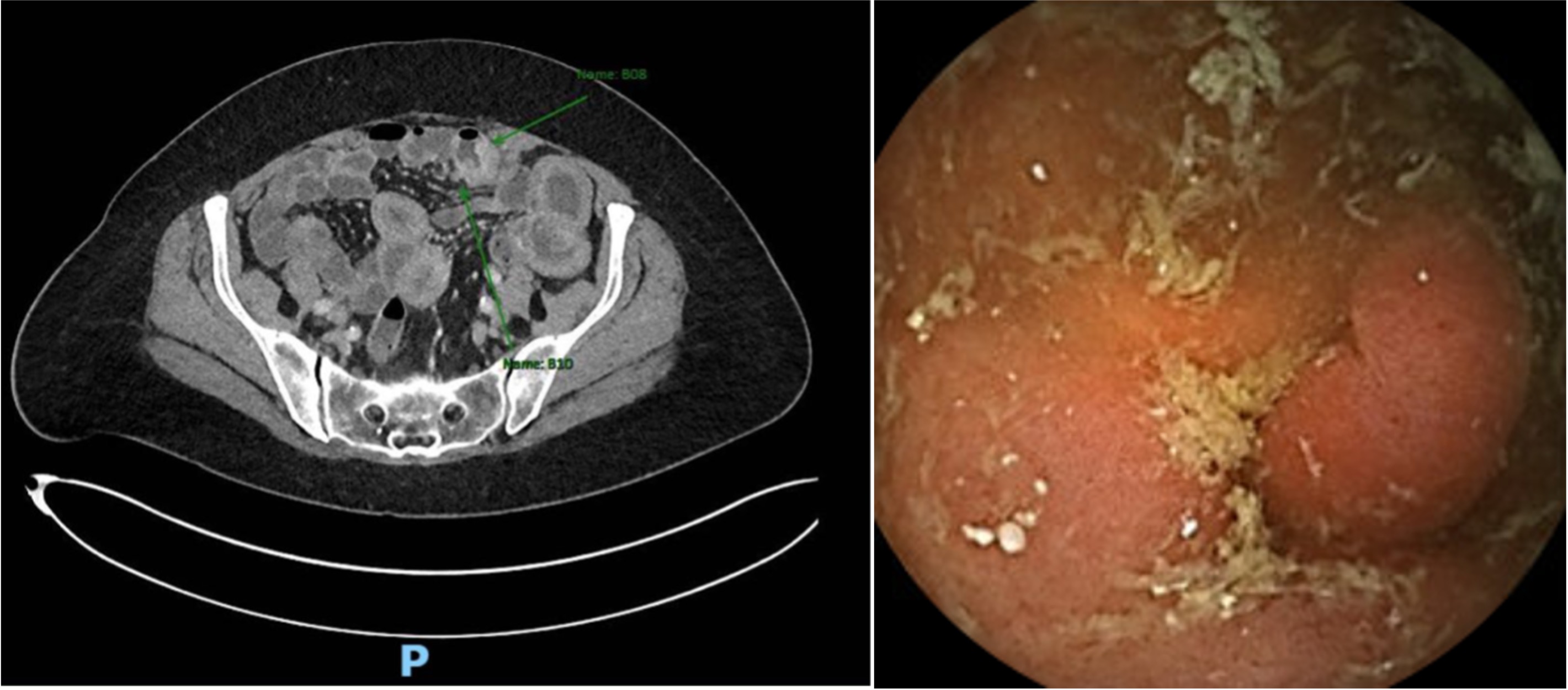
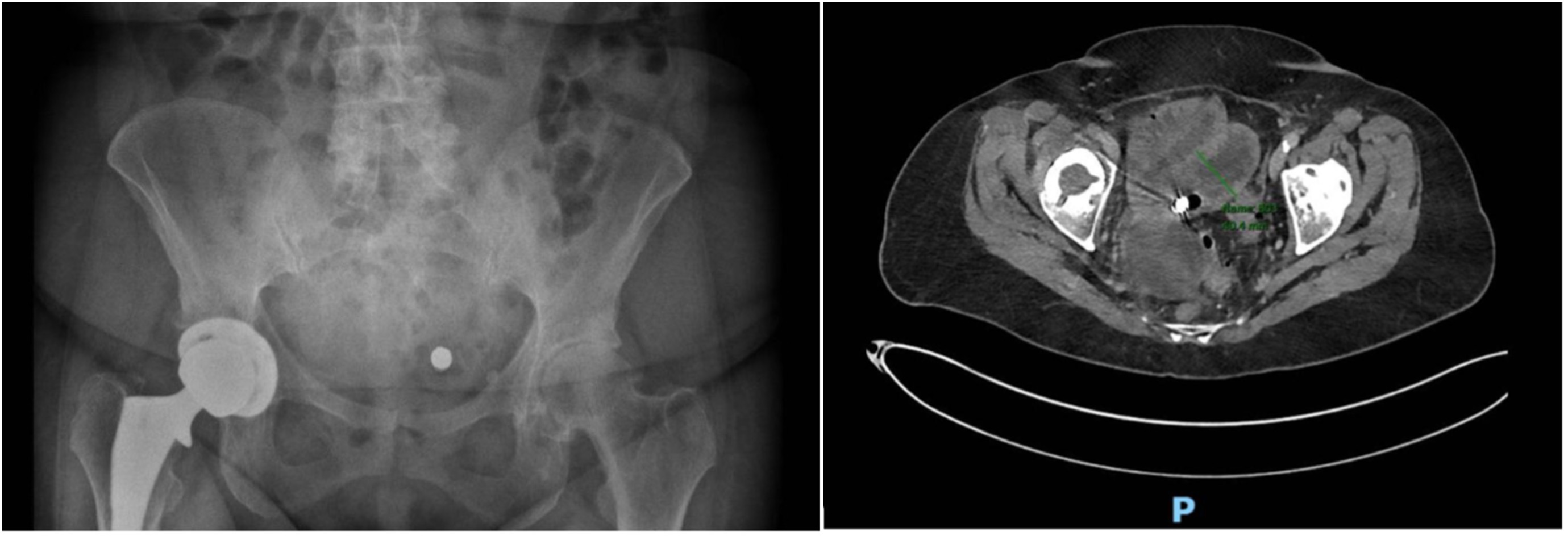
Methods: A 64-year-old female with no significant past medical history presented to the emergency department with one month of abdominal pain, nausea, vomiting, diarrhea, and 10 lb. weight loss. Recent admission to an outside hospital was notable for a negative abdominal CT, abdominal ultrasound, and esophagogastroduodenoscopy (EGD). Non-contrast CT on admission to our facility showed an SBO that gradually improved with conservative management. Colonoscopy did not reveal an underlying etiology to explain recurrent obstruction, so computed tomography enterography (CTE) was performed, which demonstrated an irregular area in the jejunum concerning for an underlying mass (Figure 1). Capsule endoscopy was requested by our surgical colleagues to help localize the lesion, as it can often be difficult to do so intra-operatively. CE revealed a small bowel mass that was difficult to fully characterize as it was seen in only a single image (Figure 1). Kidney, ureters, and bladder x-ray (KUB) (Figure 2) and repeat CTE (Figure 2) confirmed retention of the capsule and served as a target for surgical resection. Pathology showed adenocarcinoma and the patient is now receiving chemotherapy. Discussion: CE is commonly used to diagnose difficult to reach lesions but is generally contraindicated in cases where capsule retention is likely, such as in patients with known strictures or obstruction. This case illustrates the novel use of CE to localize a mass for surgical planning by allowing capsule retention to localize the obstruction through subsequent imaging. Additionally, it demonstrates the difficulty of identifying and localizing small bowel neoplasms in patients presenting with recurrent SBO.
Figure: Figure 1- Short segment of slightly nodular enhancing irregular appearing jejunal wall within the distal jejunum concerning for underlying mass with adjacent small mesenteric lymph nodes (left). CE showing potential small bowel mass. This was only visible in a single image which was not sufficient to fully characterize a possible lesion (right).
Figure: Figure 2- KUB showing retained capsule (left). Repeat CTE showed that the capsule did not pass the jejunal lesion (right).
Disclosures: Ana Lopez Alvarez indicated no relevant financial relationships. Claire Maher indicated no relevant financial relationships. Emily Minor indicated no relevant financial relationships. Rebecca Haug indicated no relevant financial relationships.
Ana S. Lopez Alvarez, BS, MS1, Claire F. Maher, BA1, Emily Minor, MD, PhD2, Rebecca Haug, MD3. P6250 - A Unique Approach to Localization of Small Bowel Neoplasm Using Capsule Endoscopy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")