HCA Healthcare Riverside Community Hospital Riverside, CA
Nishani Wickramarachchi, DO1, Raj Gulati, DO2, Regis Lee, DO1, Jennifer Hou, MD, PhD1, Alex Prevallet, DO1, Eric H. Choi, MD, FACG1 1HCA Healthcare Riverside Community Hospital, Riverside, CA; 2Riverside Community Hospital, Riverside, CA Introduction: Internal hernia and obstruction through a Petersen’s defect are complications of Roux-en-Y gastric bypass (RYGB), with an estimated incidence of 0.9-4.5%. This report details a patient with signs of acute abdomen and who was found to have an ischemic bowel due to Petersen's hernia in the setting of gastrointestinal bleed (GI).
Case Description/
Methods: Herein, we present a case of a 42-year-old woman with history of gastric sleeve converted to RYGB, who presented with fatigue and one episode of large volume coffee ground emesis. Three weeks prior, she had an upper endoscopy (EGD) performed which showed LA grade D esophagitis and a 4 cm gastrojejunostomy (GJ) large clean based ulcer which was treated with oral proton pump inhibitor (PPI) and sucralfate. She denied any NSAID use. Family history was pertinent for colon cancer in patient’s uncle and gastric cancer in a second-degree relative. Patient reported a normal colonoscopy 12 years ago.
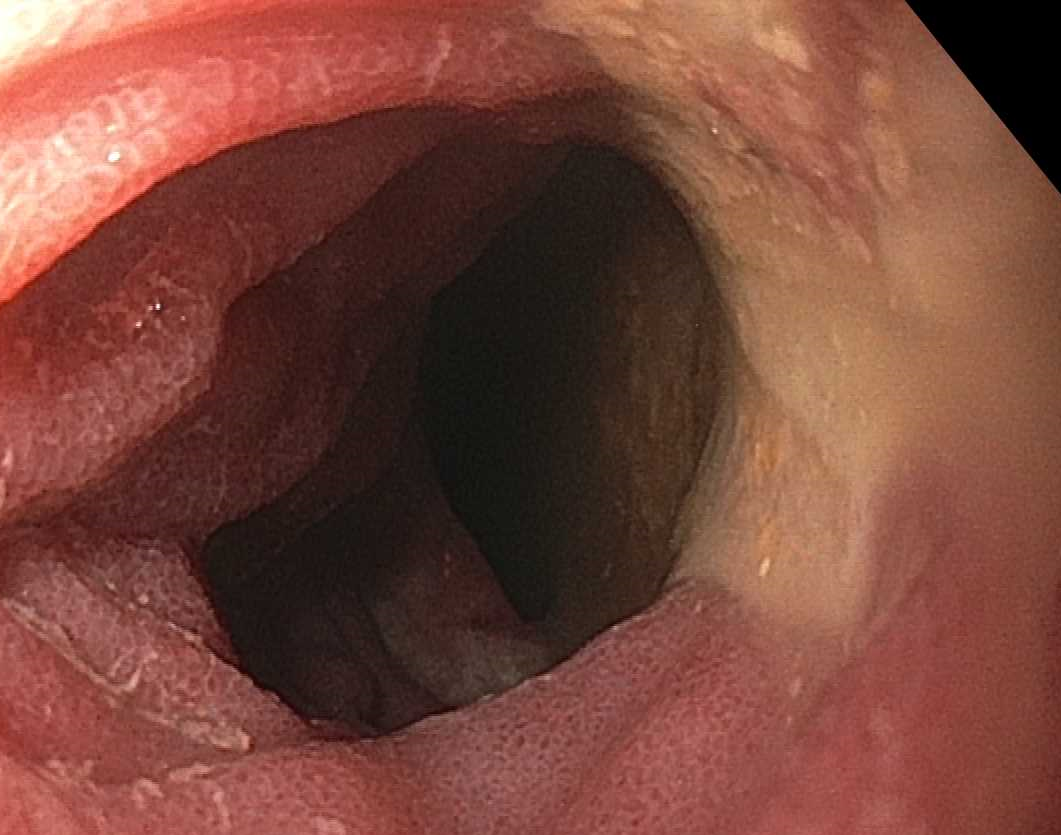
Due to her ongoing symptoms, she underwent repeat EGD which showed erythema at the GJ anastomosis, with clean based ulceration on the jejunal limb and inflamed, friable jejunal mucosa with subepithelial hemorrhage (Fig. 1). Surgery was also consulted for suspected ischemic small bowel. Exploratory laparotomy revealed a closed loop bowel obstruction internal hernia through a Petersen’s defect and a dusky appearance of the ascending limb of the jejunum. She underwent lysis of adhesions, reduction of the internal hernia, repair of the defect, and small bowel decompression. Pathology showed inflamed tissue without evidence of malignancy. Following her procedure, she remained NPO except for medications and a nasogastric tube was placed for suction. She had resolution of her symptoms, received PPI therapy and a course of antibiotics, and was discharged from the hospital with outpatient follow up. Discussion: This case highlights the diagnostic challenges of determining the etiology of GI bleeding in patients with RYGB. The patient’s coffee ground emesis may be due to bleeding from ischemic bowel through the internal hernia and/or the jejunal ulcer.
Figure: Fig. 1. Endoscopic evaluation. Upper endoscopy revealed clean based ulceration on the jejunal limb and inflamed, friable jejunal mucosa with subepithelial hemorrhage.
Disclosures: Nishani Wickramarachchi indicated no relevant financial relationships. Raj Gulati indicated no relevant financial relationships. Regis Lee indicated no relevant financial relationships. Jennifer Hou indicated no relevant financial relationships. Alex Prevallet indicated no relevant financial relationships. Eric H. Choi indicated no relevant financial relationships.
Nishani Wickramarachchi, DO1, Raj Gulati, DO2, Regis Lee, DO1, Jennifer Hou, MD, PhD1, Alex Prevallet, DO1, Eric H. Choi, MD, FACG1. P6245 - Petersen’s Hernia in the Setting of Gastrointestinal Bleeding: A Diagnostic Challenge After Roux-en-Y Gastric Bypass, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.