Thomas Jefferson University Hospital Philadelphia, PA
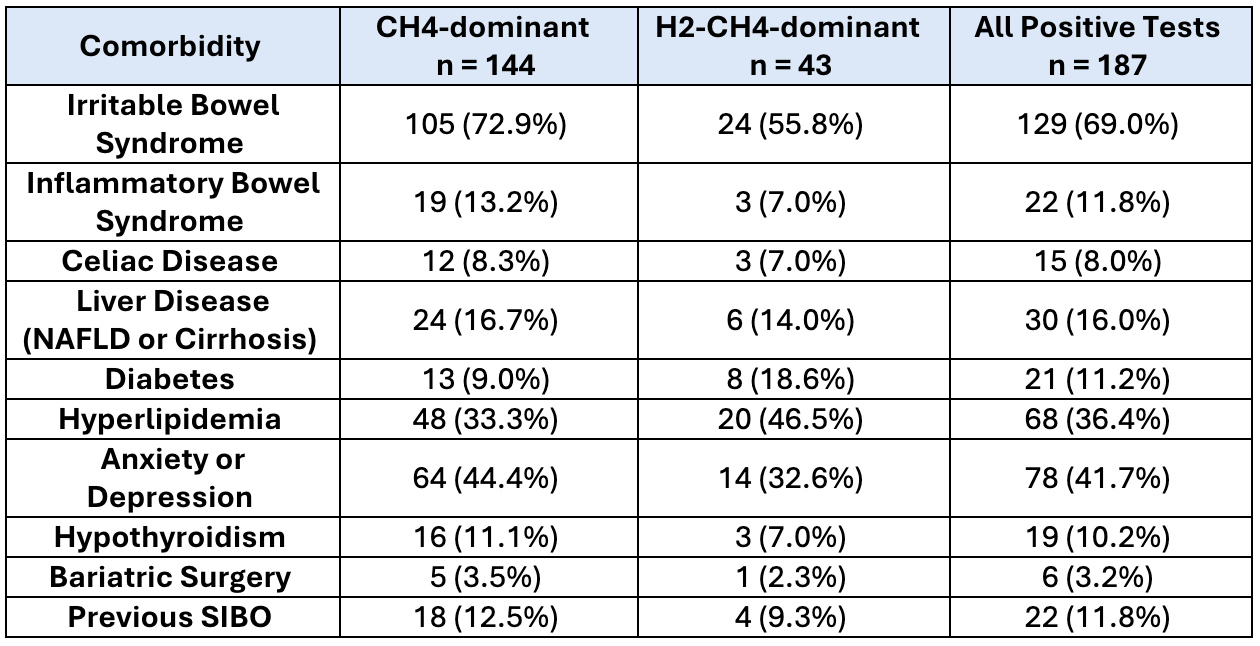
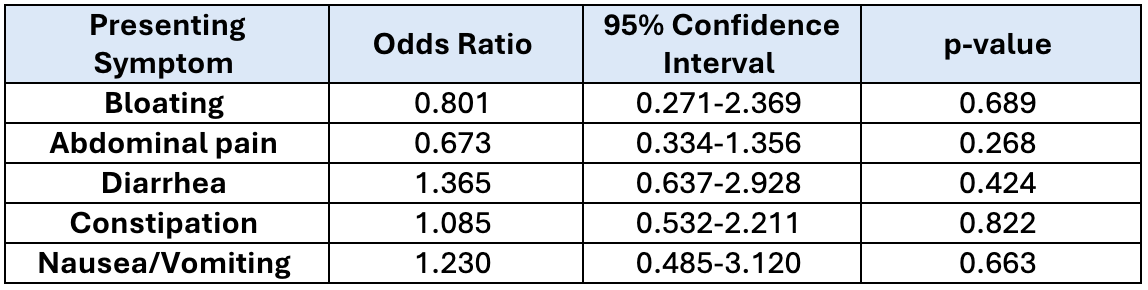
Emily Chiacchiaro, MD1, Jacqueline Krieger, MD2, Alexis Notarianni, MD1, Tammy Tran, MD1, Reeya Lele, MD3, Nicholas Fox, MD2, David Baek, BSc2, Anna Chen, MD1, Marc Hersh, MD1, Christopher Adkins, MD3, Monjur Ahmed, MD1 1Thomas Jefferson University Hospital, Philadelphia, PA; 2Sidney Kimmel Medical College at Thomas Jefferson University, Philadelphia, PA; 3Thomas Jefferson University, Philadelphia, PA Introduction: Intestinal overgrowth is identified through the lactulose breath test (LBT) and presents with nonspecific symptoms such as bloating, changes in bowel habits, or abdominal discomfort. Intestinal overgrowth can be categorized into Hydrogen-dominant (H2-dominant), Methane-dominant (CH4-dominant), and Hydrogen-Methane-Dominant (H2-CH4-dominant). Limited data exists comparing the clinical profiles of these subtypes. This study aims to evaluate the prevalence of different overgrowth subtypes and assess whether presenting symptoms can be used to predict them. Methods: We conducted a retrospective study of 213 patients who had positive LBT results at a single academic outpatient gastroenterology clinic between December 2024 and May 2025. These tests were interpreted according to the 2017 North American Consensus. Data collected included demographics, presenting symptoms (bloating, diarrhea, constipation, nausea, and abdominal pain), comorbidities, and breath test results. Logistic regression was used to calculate odds ratios for symptom-based prediction of intestinal overgrowth subtype. Results: Of 213 patients, 187 (87.8.%) tested positive for intestinal overgrowth. CH4-dominant was the most common subtype (144/213, 67.6%), followed by H2-CH4-dominant (43/213, 20.2%). No patients had isolated H2-dominant intestinal overgrowth. The cohort was predominantly female (67.2%) and white (69%). Irritable bowel syndrome (IBS) was the most common comorbidity, seen in 69% of positive cases (Table 1). Logistic regression revealed that none of the five symptoms were statistically significant predictors of overgrowth subtype (all p > .05) (Table 2). The strongest predictor was abdominal pain, with 33% lower odds in H2-CH4-dominant patients compared to CH4-dominant, though it was not significant (p = 0.268). Discussion: Symptom profiles did not significantly distinguish between CH4-dominant and H2-CH4-dominant overgrowth, underscoring the importance of objective data when making a diagnosis and treating intestinal overgrowth. Notably, CH4-dominant overgrowth was highly prevalent, while H2-dominant cases were absent. Further analysis, such as geographic distribution or microbiome composition, may be beneficial in understanding the variation in prevalence of different subtypes. While the prevalence of intestinal overgrowth in the general population remains unknown, this data indicates that a substantial proportion of patients with IBS may have concurrent intestinal overgrowth and could benefit from testing.
Figure: Table 1. Distribution of comorbidities among patients who tested positive for intestinal overgrowth by subtype.
Figure: Table 2. Association between presenting symptoms and subtype of intestinal overgrowth (CH4-Dominant vs. H2–CH4-Dominant).
Disclosures: Emily Chiacchiaro indicated no relevant financial relationships. Jacqueline Krieger indicated no relevant financial relationships. Alexis Notarianni indicated no relevant financial relationships. Tammy Tran indicated no relevant financial relationships. Reeya Lele indicated no relevant financial relationships. Nicholas Fox indicated no relevant financial relationships. David Baek indicated no relevant financial relationships. Anna Chen indicated no relevant financial relationships. Marc Hersh indicated no relevant financial relationships. Christopher Adkins indicated no relevant financial relationships. Monjur Ahmed indicated no relevant financial relationships.
Emily Chiacchiaro, MD1, Jacqueline Krieger, MD2, Alexis Notarianni, MD1, Tammy Tran, MD1, Reeya Lele, MD3, Nicholas Fox, MD2, David Baek, BSc2, Anna Chen, MD1, Marc Hersh, MD1, Christopher Adkins, MD3, Monjur Ahmed, MD1. P6212 - Subtypes of Intestinal Overgrowth in Clinical Practice: A Single Center Study, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.