Florida Atlantic University Charles E. Schmidt College of Medicine Miami, FL
Allison Chin, MD1, Gurdeep Singh, DO2, Baha Fawwaz, MD3, Mohammad Asfari, MD3, Jalal Samhoun, MD4 1Florida Atlantic University Charles E. Schmidt College of Medicine, Miami, FL; 2AdventHealth, Orlando, FL; 3Department of Gastroenterology and Hepatology, AdventHealth Orlando, Orlando, FL; 4Florida Atlantic University Charles E. Schmidt College of Medicine, Boca Raton, FL Introduction: Gastrointestinal stromal tumors (GIST) are the most common mesenchymal neoplasms of the gastrointestinal (GI) system. They originate from the interstitial cells of Cajal, and their pathogenesis is most attributed to constitutive activation of the KIT receptor tyrosine kinase gene or the platelet-derived growth factor receptor alpha (PDGFRA) gene. They are increasingly associated with extra intestinal tumors such as sarcomas and non-Hodgkin lymphoma. However, there is a gap in the literature regarding their association with primary central nervous system (CNS) neoplasms.
Case Description/
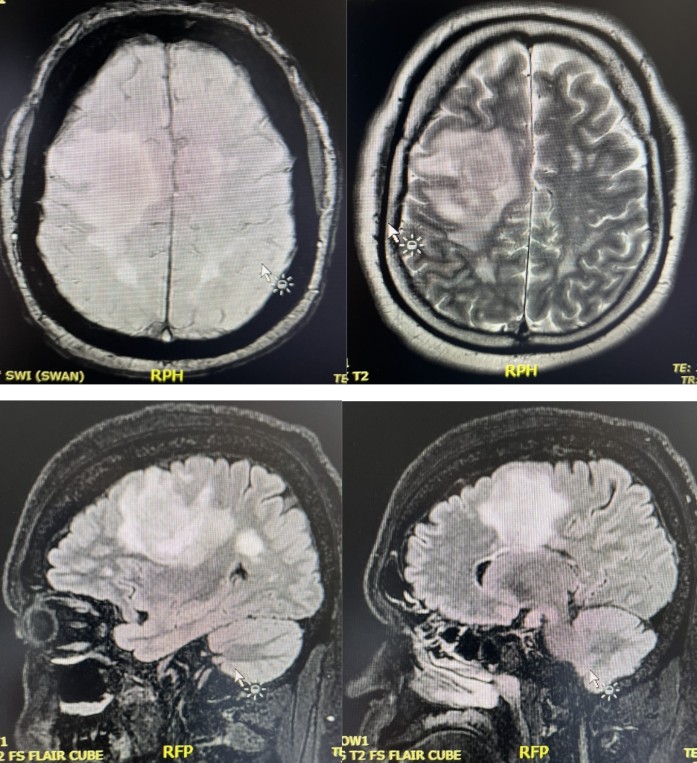
Methods: A 59-year-old male with a medical history of gastroesophageal reflux and hypertension was admitted for weakness and decreased upper extremity dexterity. He was found to have a right posterior frontal mass (5.6cm x 4.5cm x 6.1cm) with significant vasogenic edema and irregular margins with perivascular infiltration that was positive for B-cell lymphoma via image guided stereotactic biopsy. Additional imaging revealed a 4cm x 3.4cm x 4cm endophytic mass along the body of the stomach. He underwent esophagogastroduodenoscopy (EGD) which revealed a submucosal mass on the greater curvature of the gastric body and subsequently underwent endoscopic ultrasound (EUS) guided fine needle aspiration with pathology consistent with GIST. Carcinoembryonic antigen, alpha- fetoprotein, and carbohydrate antigen 19-9 were within normal range. Discussion: The purpose of this case is to highlight a unique case of a GIST tumor and a concurrent primary CNS tumor. The knee jerk reaction when identifying multiple neoplasms is to assume metastasis. However, this case emphasizes the importance of thinking outside the box to consider synchronous primary neoplasms, as primary brain tumors are derived from neuroectodermal tissue which excludes metastasis in the form of a mesenchymal tumor. Indeed, the rare possibility of a slow growing, asymptomatic GIST tumor metastasizing to the brain has been reported in about 25 cases. However, there is a gap in literature elucidating the relationship between GIST tumors and CNS B-cell lymphoma. This warrants further investigation into not only the association of GISTs with primary tumors but specifically regarding CNS B-cell lymphoma to optimize patient care, analyze prognosis, and develop novel surveillance and screening strategies for these patients.
Figure: Image 1. Axial T2 Susceptibility Weighted Angiography (SWAN) MRI (Top Left), Axial T2 Magnetic Resonance Imaging (MRI) (Top Right), and Sagittal T2 FS Fluid-Attenuated Inversion Recovery (FLAIR) Cube (Bottom) images of right posterior frontal lobe mass with significant T2 signal decrease and diffusion restriction.
Figure: Image 2: EGD with submucosal mass.
Disclosures: Allison Chin indicated no relevant financial relationships. Gurdeep Singh indicated no relevant financial relationships. Baha Fawwaz indicated no relevant financial relationships. Mohammad Asfari indicated no relevant financial relationships. Jalal Samhoun indicated no relevant financial relationships.
Allison Chin, MD1, Gurdeep Singh, DO2, Baha Fawwaz, MD3, Mohammad Asfari, MD3, Jalal Samhoun, MD4. P6208 - GIST When You Thought It Was One Tumor: The Diagnostic Dilemma of Dual Malignancies, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")